

In Vitro Testing of Scaffolds for Mesenchymal Stem Cell-Based Meniscus Tissue Engineering-Introducing a New Biocompatibility Scoring System
- PMID: 28773399
- PMCID: PMC5502969
- DOI: 10.3390/ma9040276
In Vitro Testing of Scaffolds for Mesenchymal Stem Cell-Based Meniscus Tissue Engineering-Introducing a New Biocompatibility Scoring System
Abstract
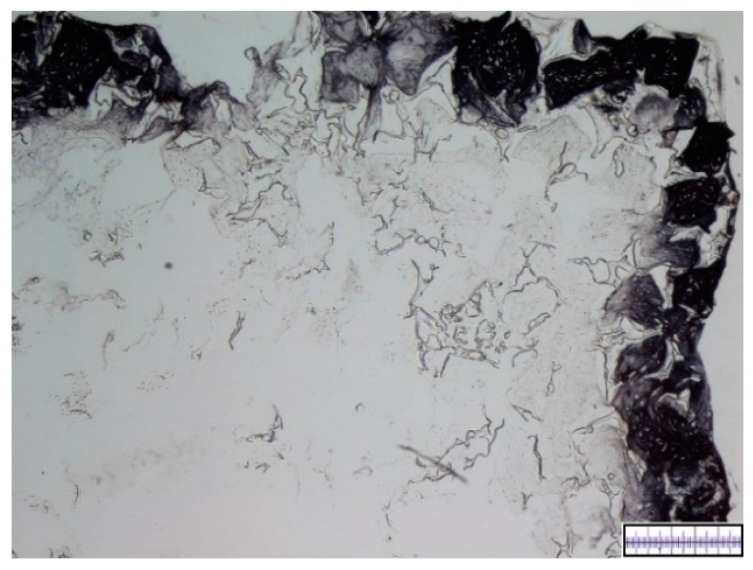
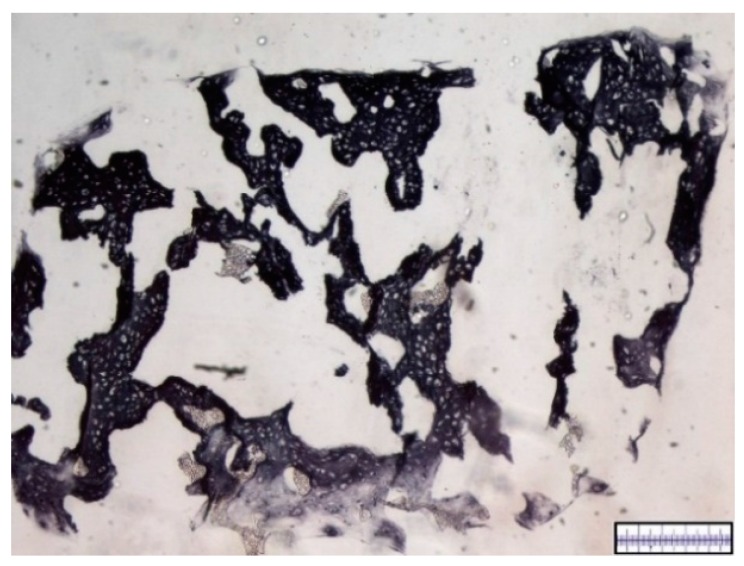
A combination of mesenchymal stem cells (MSCs) and scaffolds seems to be a promising approach for meniscus repair. To facilitate the search for an appropriate scaffold material a reliable and objective in vitro testing system is essential. This paper introduces a new scoring for this purpose and analyzes a hyaluronic acid (HA) gelatin composite scaffold and a polyurethane scaffold in combination with MSCs for tissue engineering of meniscus. The pore quality and interconnectivity of pores of a HA gelatin composite scaffold and a polyurethane scaffold were analyzed by surface photography and Berliner-Blau-BSA-solution vacuum filling. Further the two scaffold materials were vacuum-filled with human MSCs and analyzed by histology and immunohistochemistry after 21 days in chondrogenic media to determine cell distribution and cell survival as well as proteoglycan production, collagen type I and II content. The polyurethane scaffold showed better results than the hyaluronic acid gelatin composite scaffold, with signs of central necrosis in the HA gelatin composite scaffolds. The polyurethane scaffold showed good porosity, excellent pore interconnectivity, good cell distribution and cell survival, as well as an extensive content of proteoglycans and collagen type II. The polyurethane scaffold seems to be a promising biomaterial for a mesenchymal stem cell-based tissue engineering approach for meniscal repair. The new score could be applied as a new standard for in vitro scaffold testing.
Keywords: biocompatibility; chondrogenesis; collagen; composite scaffold; gelatin; human mesenchymal stem cells; hyaluronic acid; meniscus; polyurethane scaffold.
Conflict of interest statement
The authors declare no conflict of interest. Parts of the project (Actifit® biomaterial supply) were supported by Orteq. The funding sponsors had no role in the design of study; in the collection, analysis or interpretation of data; in the writing of the manuscript, and in the decision to publish the results.
Figures










References
-
- Verdonk P., Beaufils P., Bellemans J., Djian P., Heinrichs E.-L., Huysse W., Laprell H., Siebold R., Verdonk R., Colombet P., et al. Successful Treatment of Painful Irreparable Partial Meniscal Defects with a Polyurethane Scaffold: Two-Year Safety and Clinical Outcomes. Am. J. Sports Med. 2012;40:844–853. doi: 10.1177/0363546511433032. - DOI - PubMed
-
- Levy I.M., Torzilli P.A., Gould J.D., Warren R.F. The effect of lateral meniscectomy on motion of the knee. J. Bone Joint Surg. Am. 1989;71:401–406. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
