

Association of Estimated Sodium Intake With Adverse Cardiac Structure and Function: From the HyperGEN Study
- PMID: 28774377
- PMCID: PMC5571737
- DOI: 10.1016/j.jacc.2017.06.036
Association of Estimated Sodium Intake With Adverse Cardiac Structure and Function: From the HyperGEN Study
Abstract
Background: The optimal level of sodium intake remains controversial.
Objectives: This study sought to determine whether examination of left ventricular longitudinal strain (LS), circumferential strain, and e' velocity can provide insight into thresholds for the detrimental effects of estimated sodium intake (ESI) on subclinical cardiovascular disease.
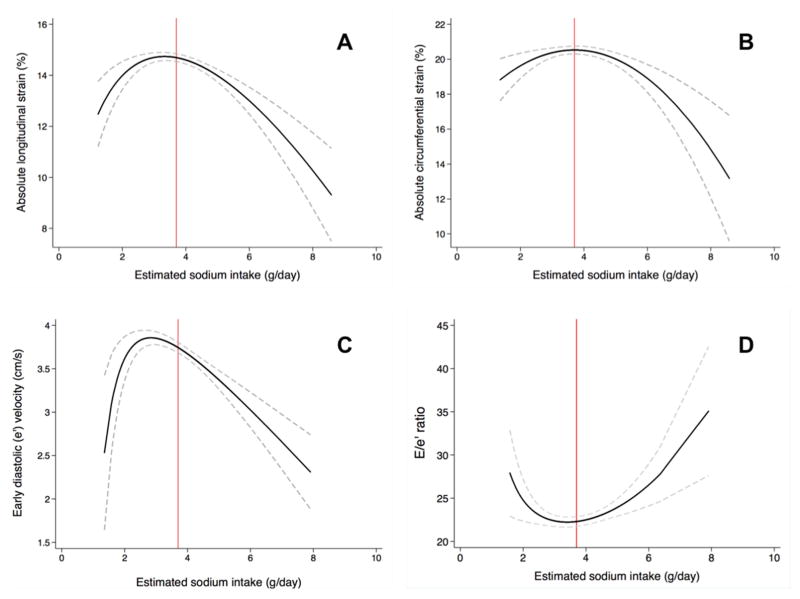
Methods: We performed speckle-tracking analysis on HyperGEN (Hypertension Genetic Epidemiology Network) study echocardiograms with available urinary sodium data (N = 2,996). We evaluated the associations among ESI and LS, circumferential strain, and e' velocity using multivariable-adjusted linear mixed-effects models (to account for relatedness among subjects) with linear splines (spline 1: ESI ≤3.7 g/day, spline 2: ESI >3.7 g/day based on visual inspection of fractional polynomial plots of the association between ESI and indices of strain and e' velocity). We performed mediation analysis to understand the indirect effects of systolic blood pressure and serum aldosterone on the relationship between ESI and strain and e' velocity.
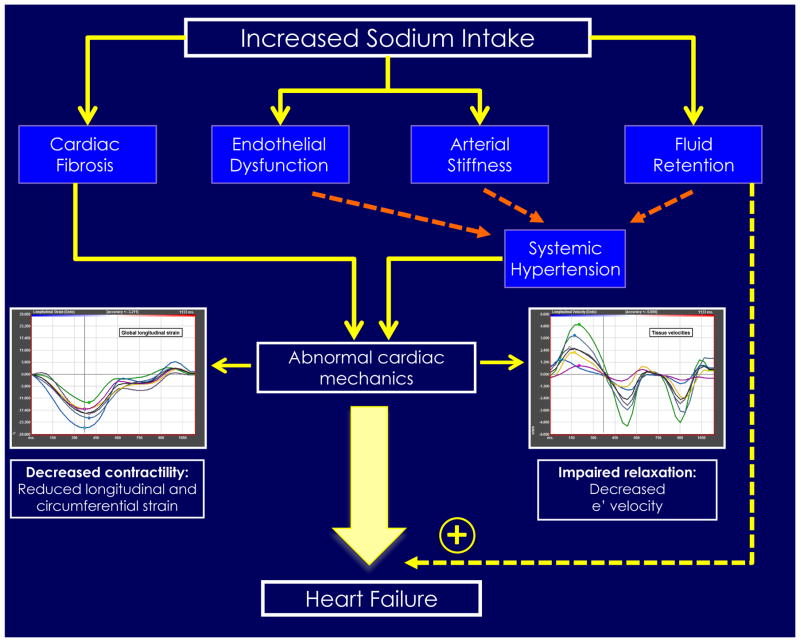
Results: Mean age of participants was 49 ± 14 years, 57% were female, 50% were African American, and 54% had hypertension. The median ESI was 3.73 (interquartile range: 3.24, 4.25) g/day. ESI >3.7 g/day was associated with larger left atrial and left ventricular dimensions (p < 0.05). After adjusting for speckle-tracking analyst, image quality, study site, age, sex, smoking status, alcohol use, daily blocks walked, diuretic use, estimated glomerular filtration rate, left ventricular mass, ejection fraction, and wall motion score index, ESI >3.7 g/day was associated with both strain parameters and e' velocity (p < 0.05 for all comparisons), but ESI ≤3.7 g/day was not (p > 0.05 for all comparisons). There were significant interactions by potassium excretion for circumferential strain. Mediation analysis suggested that systolic blood pressure explained 14% and 20% of the indirect effects between ESI and LS and e' velocity, respectively, whereas serum aldosterone explained 19% of the indirect effects between ESI and LS.
Conclusions: ESI >3.7 g/day is associated with adverse cardiac remodeling and worse systolic strain and diastolic e' velocity.
Keywords: echocardiography; sodium intake; strain; urinary sodium.
Copyright © 2017 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Sodium and Myocardial Function: An Unsavory Story.J Am Coll Cardiol. 2017 Aug 8;70(6):725-727. doi: 10.1016/j.jacc.2017.06.041. J Am Coll Cardiol. 2017. PMID: 28774378 No abstract available.
References
-
- Mente A, O’Donnell MJ, Dagenais G, et al. Validation and comparison of three formulae to estimate sodium and potassium excretion from a single morning fasting urine compared to 24-h measures in 11 countries. J Hypertens. 2014;32:1005–14. discussion 1015. - PubMed
-
- O’Donnell M, Mente A, Rangarajan S, et al. Urinary sodium and potassium excretion, mortality, and cardiovascular events. N Engl J Med. 2014;371:612–23. - PubMed
-
- Eckel RH, Jakicic JM, Ard JD, et al. 2013 AHA/ACC guideline on lifestyle management to reduce cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129:S76–99. - PubMed
-
- Guideline: Sodium Intake for Adults and Children. Geneva: 2012. - PubMed
-
- Graudal N, Jurgens G, Baslund B, Alderman MH. Compared with usual sodium intake, low- and excessive-sodium diets are associated with increased mortality: a meta-analysis. Am J Hypertens. 2014;27:1129–37. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U10 HL054509/HL/NHLBI NIH HHS/United States
- R01 HL127028/HL/NHLBI NIH HHS/United States
- P30 DK079626/DK/NIDDK NIH HHS/United States
- R01 HL107577/HL/NHLBI NIH HHS/United States
- U10 HL054473/HL/NHLBI NIH HHS/United States
- U01 HL054495/HL/NHLBI NIH HHS/United States
- U10 HL054472/HL/NHLBI NIH HHS/United States
- U01 HL054472/HL/NHLBI NIH HHS/United States
- U01 HL054471/HL/NHLBI NIH HHS/United States
- U01 HL054496/HL/NHLBI NIH HHS/United States
- U10 HL054497/HL/NHLBI NIH HHS/United States
- U01 HL054497/HL/NHLBI NIH HHS/United States
- U01 HL054509/HL/NHLBI NIH HHS/United States
- U10 HL054495/HL/NHLBI NIH HHS/United States
- U10 HL054496/HL/NHLBI NIH HHS/United States
- U10 HL054471/HL/NHLBI NIH HHS/United States
- R01 HL055673/HL/NHLBI NIH HHS/United States
- U01 HL054473/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
