

Cerebrovascular and ventilatory responses to acute normobaric hypoxia in girls and women
- PMID: 28774953
- PMCID: PMC5555897
- DOI: 10.14814/phy2.13372
Cerebrovascular and ventilatory responses to acute normobaric hypoxia in girls and women
Abstract
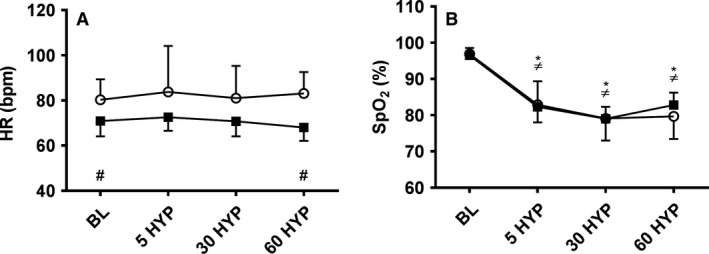
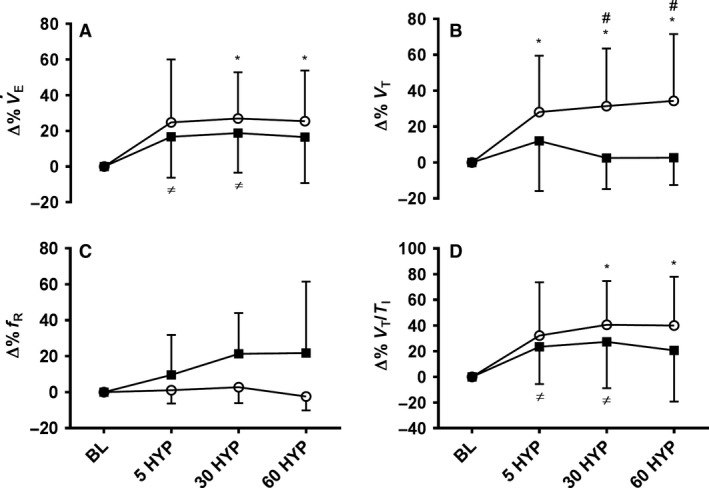
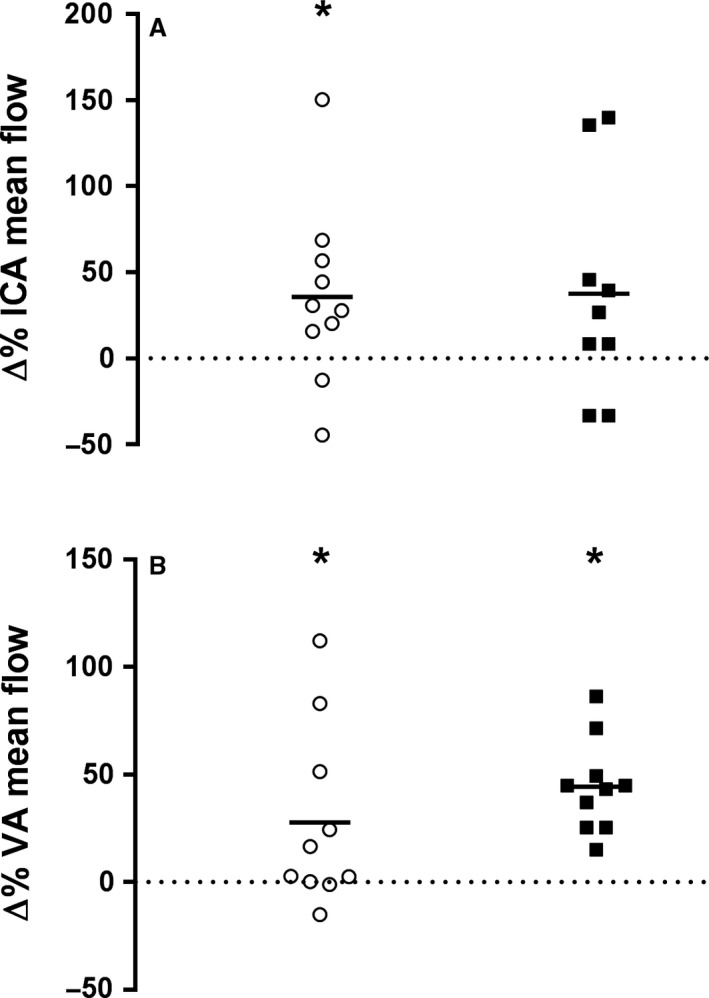
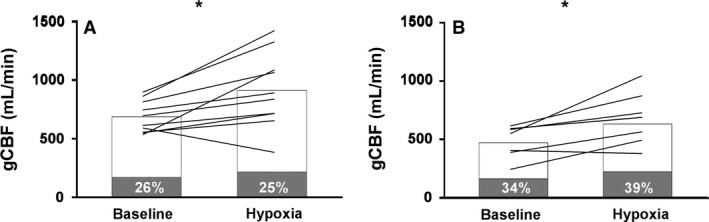
Physiological responses to hypoxia in children are incompletely understood. We aimed to characterize cerebrovascular and ventilatory responses to normobaric hypoxia in girls and women. Ten healthy girls (9.9 ± 1.7 years; mean ± SD; Tanner stage 1 and 2) and their mothers (43.9 ± 3.5 years) participated. Internal carotid (ICA) and vertebral artery (VA) velocity, diameter and flow (Duplex ultrasound) was recorded pre- and post-1 h of hypoxic exposure (FIO2 = 0.126;~4000 m) in a normobaric chamber. Ventilation (V˙E) and respiratory drive (VT/TI) expressed as delta change from baseline (∆%), and end-tidal carbon-dioxide (PETCO2) were collected at baseline (BL) and 5, 30 and 60 min of hypoxia (5/30/60 HYP). Heart rate (HR) and oxygen saturation (SpO2) were also collected at these time-points. SpO2 declined similarly in girls (BL-97%; 60HYP-80%, P < 0.05) and women (BL-97%; 60HYP-83%, P < 0.05). Global cerebral blood flow (gCBF) increased in both girls (BL-687; 60HYP-912 mL·min-1, P < 0.05) and women (BL-472; 60HYP-651 mL·min-1, P < 0.01), though the ratio of ICA:VA (%) contribution to gCBF differed significantly (girls, 75:25%; women, 61:39%). The relative increase in V˙E peaked at 30HYP in both girls (27%, P < 0.05) and women (19%, P < 0.05), as did ∆%VT/TI (girls, 41%; women, 27%, P's < 0.05). Tidal volume (VT) increased in both girls and women at 5HYP, remaining elevated above baseline in girls at 30 and 60 HYP, but declined back toward baseline in women. Girls elicit similar increases in gCBF and ventilatory parameters in response to acute hypoxia as women, though the pattern and contributions mediating these responses appear developmentally divergent.
Keywords: Cerebral perfusion; children; hypoxia; respiratory drive; ventilation.
© 2017 The Authors. Physiological Reports published by Wiley Periodicals, Inc. on behalf of The Physiological Society and the American Physiological Society.
Figures
References
-
- Ainslie, P. N. , and Hoiland R. L.. 2014. Transcranial Doppler ultrasound: valid, invalid, or both? J. Appl. Physiol. 117:1081–1083. - PubMed
-
- Cooper, D. M. , Kaplan M. R., Baumgarten L., Weiler‐Ravell D., Whipp B. J., and Wasserman K.. 1987. Coupling of ventilation and CO2 production during exercise in children. Pediatr. Res. 21:568–572. - PubMed
-
- Gaultier, C. L. , Perret L., Boule M., Buvry A., and Girard F.. 1981. Occlusion pressure and breathing pattern in healthy children. Respir. Physiol. 46:71–80. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
