

Oestrogen inhibition reverses pulmonary arterial hypertension and associated metabolic defects
- PMID: 28775043
- PMCID: PMC6532788
- DOI: 10.1183/13993003.02337-2016
Oestrogen inhibition reverses pulmonary arterial hypertension and associated metabolic defects
Abstract
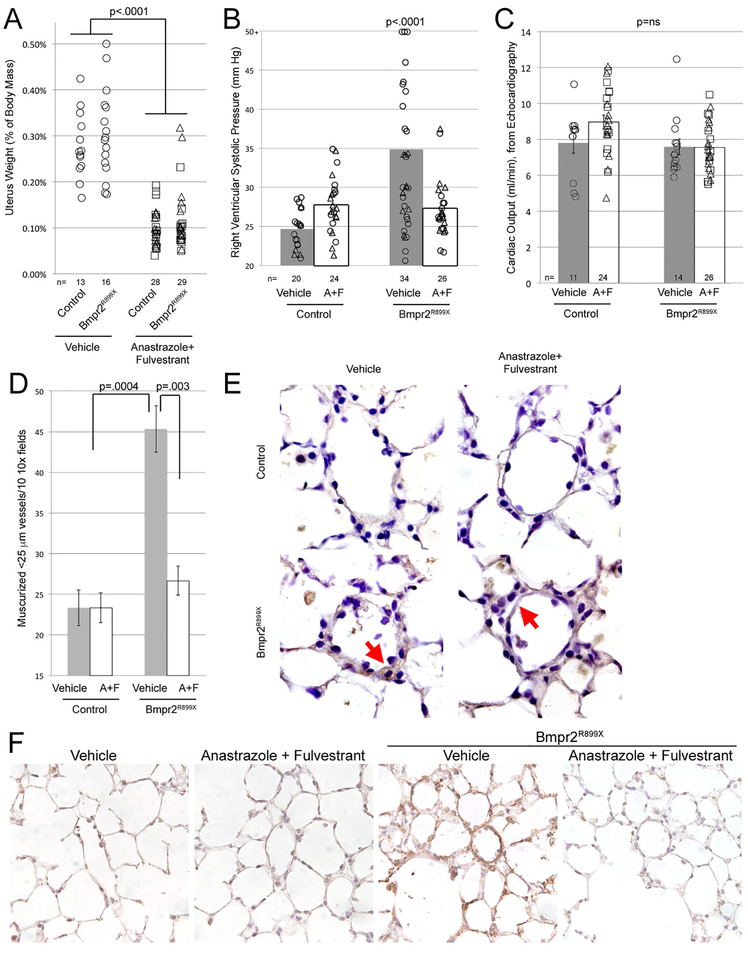
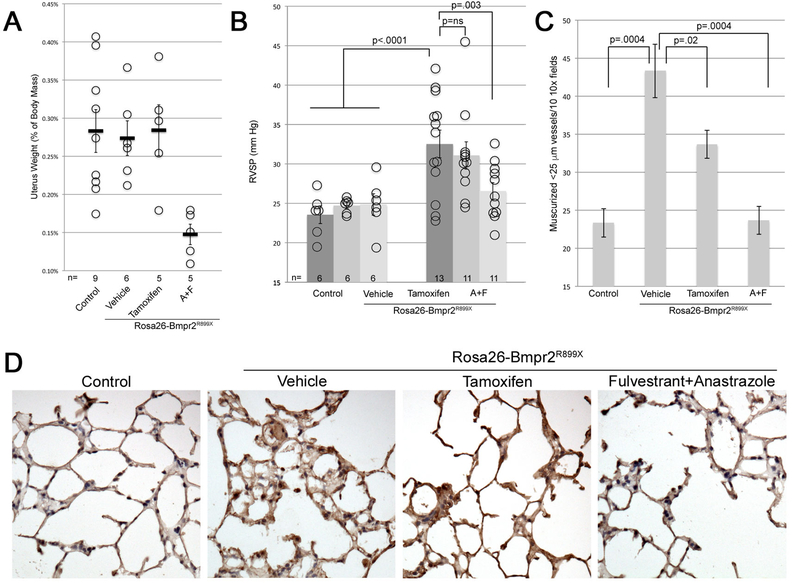
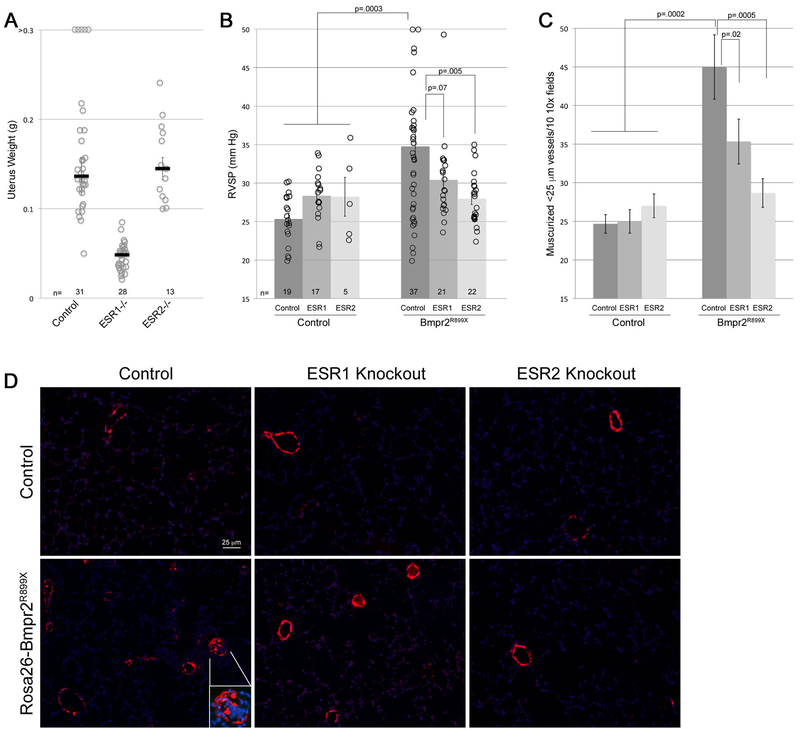
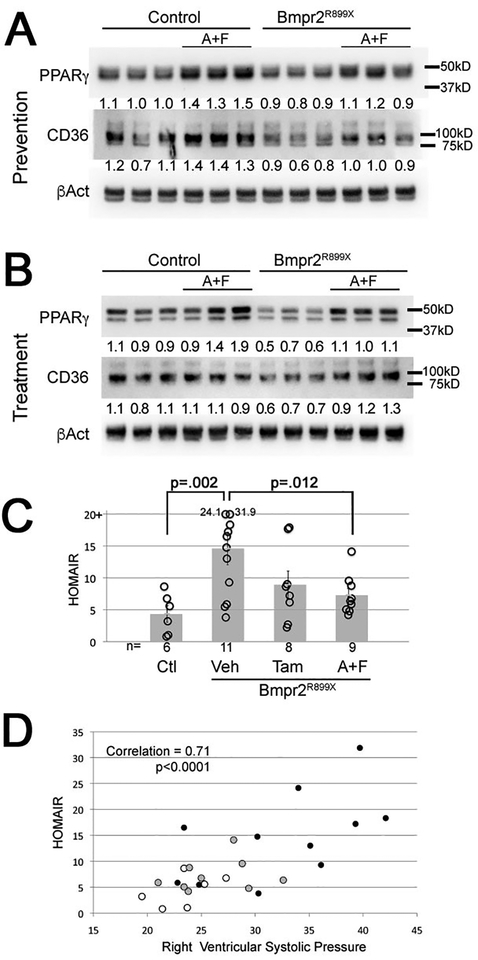
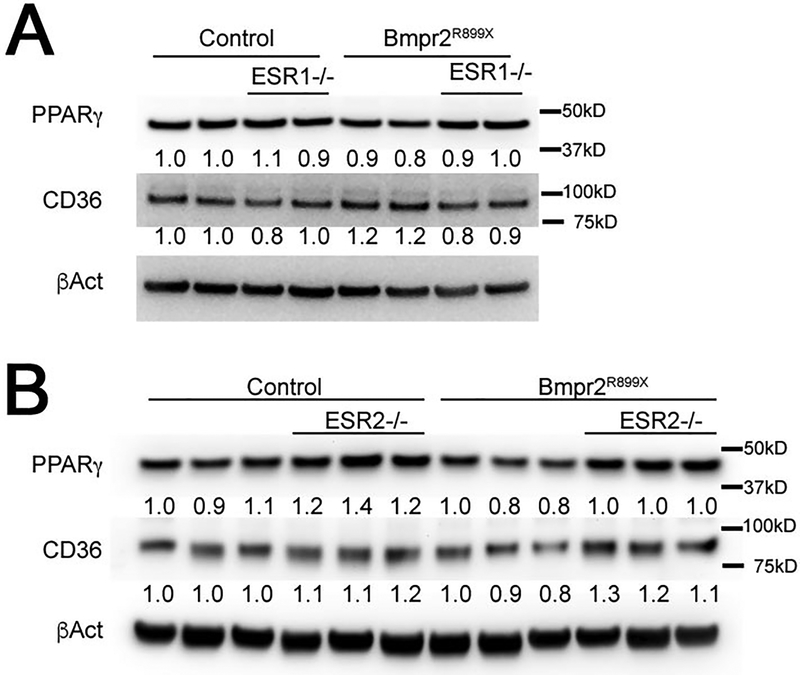
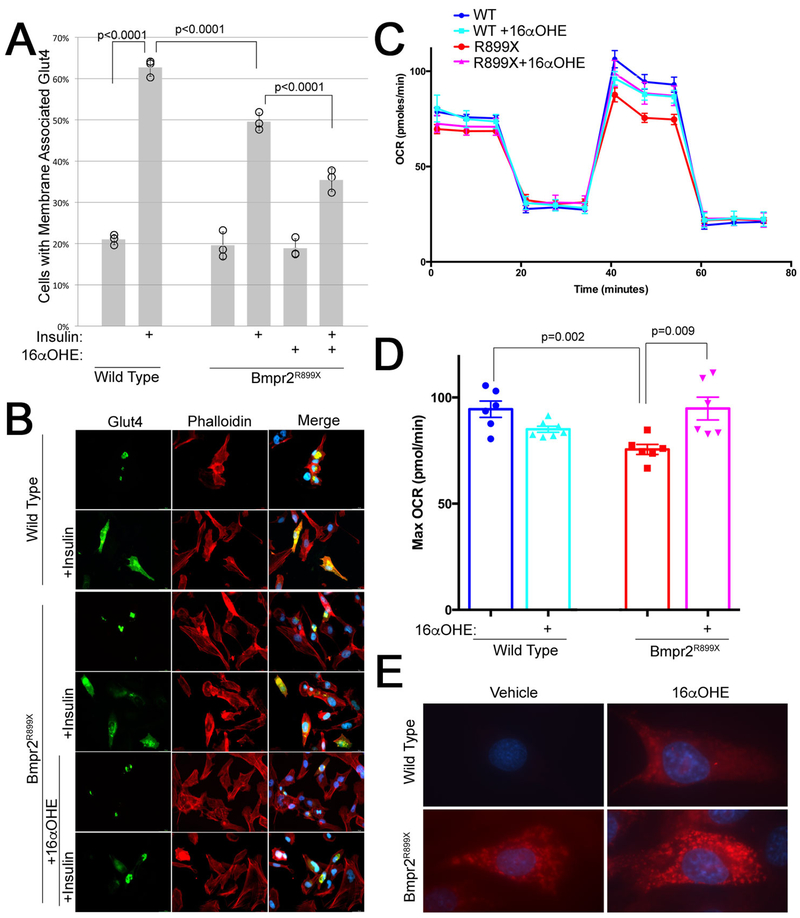
Increased oestrogen is a strong epidemiological risk factor for development of pulmonary arterial hypertension (PAH) in patients, associated with metabolic defects. In addition, oestrogens drive penetrance in mice carrying mutations in bone morphogenetic protein receptor type II (BMPR2), the cause of most heritable PAH. The goal of the present study was to determine whether inhibition of oestrogens was effective in the treatment of PAH in these mice.The oestrogen inhibitors fulvestrant and anastrozole were used in a prevention and treatment paradigm in BMPR2 mutant mice, and tamoxifen was used for treatment. In addition, BMPR2 mutant mice were crossed onto oestrogen receptor (ESR)1 and ESR2 knockout backgrounds to assess receptor specificity. Haemodynamic and metabolic outcomes were measured.Oestrogen inhibition both prevented and treated PAH in BMPR2 mutant mice. This was associated with reduction in metabolic defects including oxidised lipid formation, insulin resistance and rescue of peroxisome proliferator-activated receptor-γ and CD36. The effect was mediated primarily through ESR2, but partially through ESR1.Our data suggest that trials of oestrogen inhibition in human PAH are warranted, and may improve pulmonary vascular disease through amelioration of metabolic defects. Although fulvestrant and anastrozole were more effective than tamoxifen, tamoxifen may be useful in premenopausal females, because of a reduced risk of induction of menopause.
Copyright ©ERS 2017.
Conflict of interest statement
Conflict of interest: Disclosures can be found alongside this article at erj.ersjournals.com
Figures
Comment in
-
Inhibiting oestrogen signalling in pulmonary arterial hypertension: sex, drugs and research.Eur Respir J. 2017 Aug 3;50(2):1700983. doi: 10.1183/13993003.00983-2017. Print 2017 Aug. Eur Respir J. 2017. PMID: 28775051 No abstract available.
References
-
- de Jesus Perez VA. Molecular pathogenesis and current pathology of pulmonary hypertension. Heart Fail Rev 2015: 19. - PubMed
-
- Cogan JD, Vnencak-Jones CL, Phillips JA, 3rd, Lane KB, Wheeler LA, Robbins IM, Garrison G, Hedges LK, Loyd JE. Gross BMPR2 gene rearrangements constitute a new cause for primary pulmonary hypertension. Genet Med 2005: 7(3): 169–174. - PubMed
-
- Rajkumar R, Konishi K, Richards TJ, Ishizawar DC, Wiechert AC, Kaminski N, Ahmad F. Genomewide RNA expression profiling in lung identifies distinct signatures in idiopathic pulmonary arterial hypertension and secondary pulmonary hypertension. Am J Physiol Heart Circ Physiol 2010: 298(4): H1235–1248. - PMC - PubMed
-
- West J, Fagan K, Steudel W, Fouty B, Lane K, Harral J, Hoedt-Miller M, Tada Y, Ozimek J, Tuder R, Rodman DM. Pulmonary hypertension in transgenic mice expressing a dominant-negative BMPRII gene in smooth muscle. Circ Res 2004: 94(8): 1109–1114. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous