

Association of High-Density Lipoprotein-Cholesterol Versus Apolipoprotein A-I With Risk of Coronary Heart Disease: The European Prospective Investigation Into Cancer-Norfolk Prospective Population Study, the Atherosclerosis Risk in Communities Study, and the Women's Health Study
- PMID: 28775061
- PMCID: PMC5586475
- DOI: 10.1161/JAHA.117.006636
Association of High-Density Lipoprotein-Cholesterol Versus Apolipoprotein A-I With Risk of Coronary Heart Disease: The European Prospective Investigation Into Cancer-Norfolk Prospective Population Study, the Atherosclerosis Risk in Communities Study, and the Women's Health Study
Abstract
Background: The contribution of apolipoprotein A-I (apoA-I) to coronary heart disease (CHD) risk stratification over and above high-density lipoprotein cholesterol (HDL-C) is unclear. We studied the associations between plasma levels of HDL-C and apoA-I, either alone or combined, with risk of CHD events and cardiovascular risk factors among apparently healthy men and women.
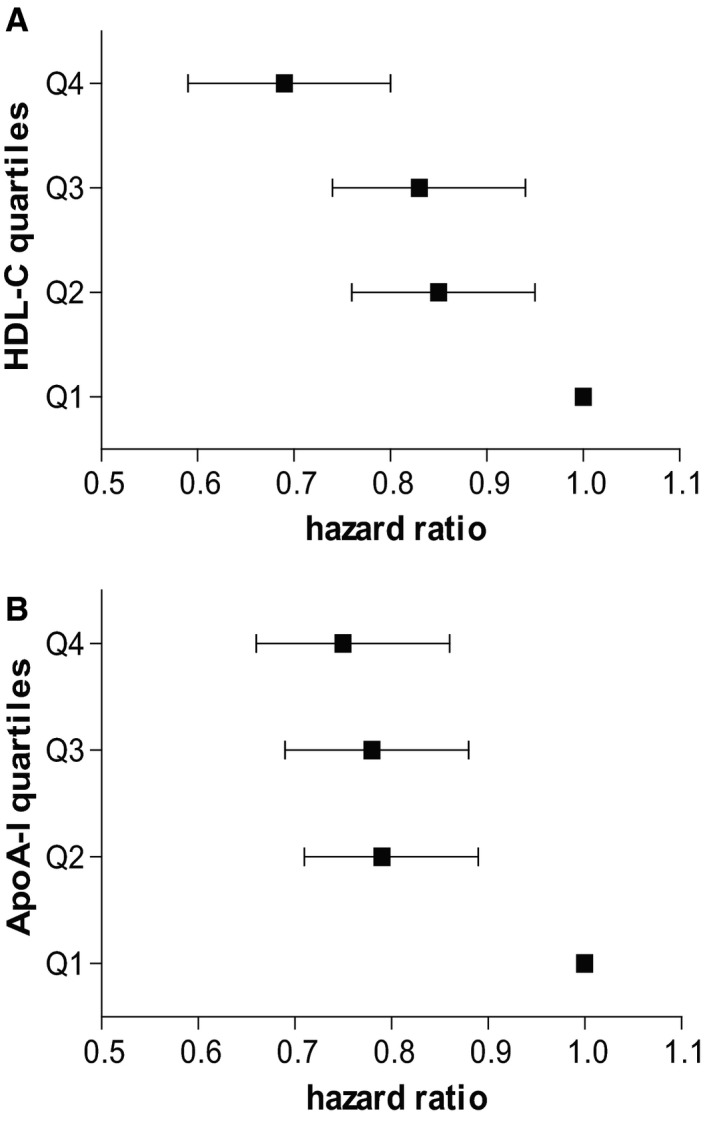
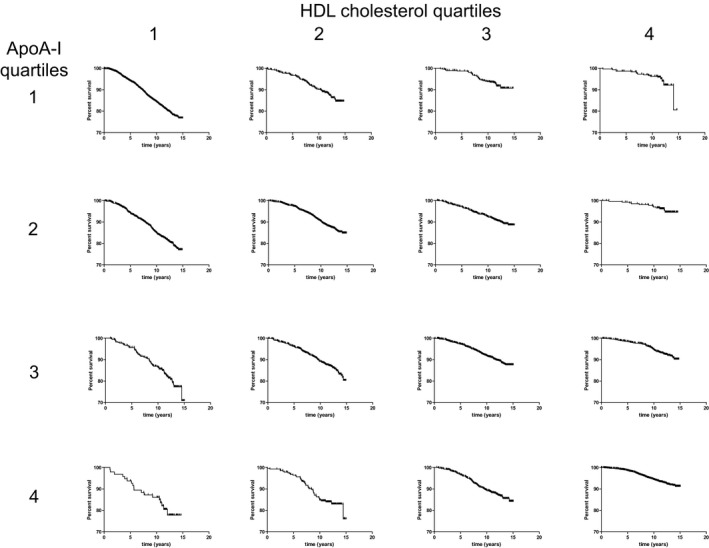
Methods and results: HDL-C and apoA-I levels were measured among 17 661 participants of the EPIC (European Prospective Investigation into Cancer)-Norfolk prospective population study. Hazard ratios for CHD events and distributions of risk factors were calculated by quartiles of HDL-C and apoA-I. Results were validated using data from the ARIC (Atherosclerosis Risk in Communities) and WHS (Women's Health Study) cohorts, comprising 15 494 and 27 552 individuals, respectively. In EPIC-Norfolk, both HDL-C and apoA-I quartiles were strongly and inversely associated with CHD risk. Within HDL-C quartiles, higher apoA-I levels were not associated with lower CHD risk; in fact, CHD risk was higher within some HDL-C quartiles. ApoA-I levels were associated with higher levels of CHD risk factors: higher body mass index, HbA1c, non-HDL-C, triglycerides, apolipoprotein B, systolic blood pressure, and C-reactive protein, within fixed HDL-C quartiles. In contrast, HDL-C levels were consistently inversely associated with overall CHD risk and CHD risk factors within apoA-I quartiles (P<0.001). These findings were validated in the ARIC and WHS cohorts.
Conclusions: Our findings demonstrate that apoA-I levels do not offer predictive information over and above HDL-C. In fact, within some HDL-C quartiles, higher apoA-I levels were associated with higher risk of CHD events, possibly because of the unexpected higher prevalence of cardiovascular risk factors in association with higher apoA-I levels.
Clinical trial registration: URL: https://www.clinicaltrials.gov. Unique identifier: NCT00000479.
Keywords: apolipoprotein A‐I; cardiovascular disease; coronary heart disease; high‐density lipoprotein cholesterol.
© 2017 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
Similar articles
-
High-density lipoprotein cholesterol, high-density lipoprotein particle size, and apolipoprotein A-I: significance for cardiovascular risk: the IDEAL and EPIC-Norfolk studies.J Am Coll Cardiol. 2008 Feb 12;51(6):634-42. doi: 10.1016/j.jacc.2007.09.060. J Am Coll Cardiol. 2008. PMID: 18261682 Clinical Trial.
-
Non-HDL cholesterol vs. apo B for risk of coronary heart disease in healthy individuals: the EPIC-Norfolk prospective population study.Eur J Clin Invest. 2013 Oct;43(10):1009-15. doi: 10.1111/eci.12129. Epub 2013 Jul 17. Eur J Clin Invest. 2013. PMID: 23859101
-
Lipid assessment, metabolic syndrome and coronary heart disease risk.Eur J Clin Invest. 2010 Dec;40(12):1081-93. doi: 10.1111/j.1365-2362.2010.02357.x. Eur J Clin Invest. 2010. PMID: 20701625
-
The role of non-HDL cholesterol in risk stratification for coronary artery disease.Curr Atheroscler Rep. 2012 Apr;14(2):130-4. doi: 10.1007/s11883-011-0224-x. Curr Atheroscler Rep. 2012. PMID: 22203405 Review.
-
ApoA-I Infusion Therapies Following Acute Coronary Syndrome: Past, Present, and Future.Curr Atheroscler Rep. 2022 Jul;24(7):585-597. doi: 10.1007/s11883-022-01025-7. Epub 2022 May 7. Curr Atheroscler Rep. 2022. PMID: 35524914 Free PMC article. Review.
Cited by
-
Creation of Cybrid Cultures Containing mtDNA Mutations m.12315G>A and m.1555G>A, Associated with Atherosclerosis.Biomolecules. 2019 Sep 18;9(9):499. doi: 10.3390/biom9090499. Biomolecules. 2019. PMID: 31540444 Free PMC article.
-
Association between the Plasma-Glycosylated Hemoglobin A1c/High-Density Lipoprotein Cholesterol Ratio and Carotid Atherosclerosis: A Retrospective Study.J Diabetes Res. 2021 Nov 10;2021:9238566. doi: 10.1155/2021/9238566. eCollection 2021. J Diabetes Res. 2021. PMID: 34805413 Free PMC article.
-
U-shaped relationship between apolipoprotein A1 levels and mortality risk in men and women.Eur J Prev Cardiol. 2023 Mar 1;30(4):293-304. doi: 10.1093/eurjpc/zwac263. Eur J Prev Cardiol. 2023. PMID: 36351048 Free PMC article.
-
Photodynamic Therapy for Atherosclerosis.Int J Mol Sci. 2024 Feb 6;25(4):1958. doi: 10.3390/ijms25041958. Int J Mol Sci. 2024. PMID: 38396639 Free PMC article. Review.
-
Cholesterol Acceptors Regulate the Lipidome of Macrophage Foam Cells.Int J Mol Sci. 2019 Aug 2;20(15):3784. doi: 10.3390/ijms20153784. Int J Mol Sci. 2019. PMID: 31382484 Free PMC article.
References
-
- Voight BF, Peloso GM, Orho‐Melander M, Frikke‐Schmidt R, Barbalic M, Jensen MK, Hindy G, Hólm H, Ding EL, Johnson T, Schunkert H, Samani NJ, Clarke R, Hopewell JC, Thompson JF, Li M, Thorleifsson G, Newton‐Cheh C, Musunuru K, Pirruccello JP, Saleheen D, Chen L, Stewart AF, Schillert A, Thorsteinsdottir U, Thorgeirsson G, Anand S, Engert JC, Morgan T, Spertus J, Stoll M, Berger K, Martinelli N, Girelli D, McKeown PP, Patterson CC, Epstein SE, Devaney J, Burnett M‐S, Mooser V, Ripatti S, Surakka I, Nieminen MS, Sinisalo J, Lokki M‐L, Perola M, Havulinna A, de Faire U, Gigante B, Ingelsson E, Zeller T, Wild P, de Bakker PIW, Klungel OH, Maitland‐van der Zee A‐H, Peters BJM, de Boer A, Grobbee DE, Kamphuisen PW, Deneer VHM, Elbers CC, Onland‐Moret NC, Hofker MH, Wijmenga C, Verschuren WM, Boer JM, van der Schouw YT, Rasheed A, Frossard P, Demissie S, Willer C, Do R, Ordovas JM, Abecasis GR, Boehnke M, Mohlke KL, Daly MJ, Guiducci C, Burtt NP, Surti A, Gonzalez E, Purcell S, Gabriel S, Marrugat J, Peden J, Erdmann J, Diemert P, Willenborg C, König IR, Fischer M, Hengstenberg C, Ziegler A, Buysschaert I, Lambrechts D, Van de Werf F, Fox KA, El Mokhtari NE, Rubin D, Schrezenmeir J, Schreiber S, Schäfer A, Danesh J, Blankenberg S, Roberts R, McPherson R, Watkins H, Hall AS, Overvad K, Rimm E, Boerwinkle E, Tybjaerg‐Hansen A, Cupples LA, Reilly MP, Melander O, Mannucci PM, Ardissino D, Siscovick D, Elosua R, Stefansson K, O'Donnell CJ, Salomaa V, Rader DJ, Peltonen L, Schwartz SM, Altshuler D, Kathiresan S. Plasma HDL cholesterol and risk of myocardial infarction: a Mendelian randomisation study. Lancet. 2012;380:572–580. - PMC - PubMed
-
- Boden WE, Probstfield JL, Anderson T, Chaitman BR, Desvignes‐Nickens P, Koprowicz K, McBride R, Teo K, Weintraub W. Niacin in patients with low HDL cholesterol levels receiving intensive statin therapy. N Engl J Med. 2011;365:2255–2267. - PubMed
-
- Schwartz GG, Olsson AG, Abt M, Ballantyne CM, Barter PJ, Brumm J, Chaitman BR, Holme IM, Kallend D, Leiter LA, Leitersdorf E, McMurray JJ, Mundl H, Nicholls SJ, Shah PK, Tardif J‐C, Wright RS. Effects of dalcetrapib in patients with a recent acute coronary syndrome. N Engl J Med. 2012;367:2089–2099. - PubMed
-
- Lincoff AM, Nicholls SJ, Riesmeyer JS, Barter PJ, Brewer HB, Fox KAA, Gibson CM, Granger C, Menon V, Montalescot G, Rader D, Tall AR, McErlean E, Wolski K, Ruotolo G, Vangerow B, Weerakkody G, Goodman SG, Conde D, McGuire DK, Nicolau JC, Leiva‐Pons JL, Pesant Y, Li W, Kandath D, Kouz S, Tahirkheli N, Mason D, Nissen SE; ACCELERATE Investigators . Evacetrapib and cardiovascular outcomes in high‐risk vascular disease. N Engl J Med. 2017;376:1933–1942. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
