

Relationship between haemodynamic impairment and collateral blood flow in carotid artery disease
- PMID: 28776469
- PMCID: PMC6238174
- DOI: 10.1177/0271678X17724027
Relationship between haemodynamic impairment and collateral blood flow in carotid artery disease
Abstract
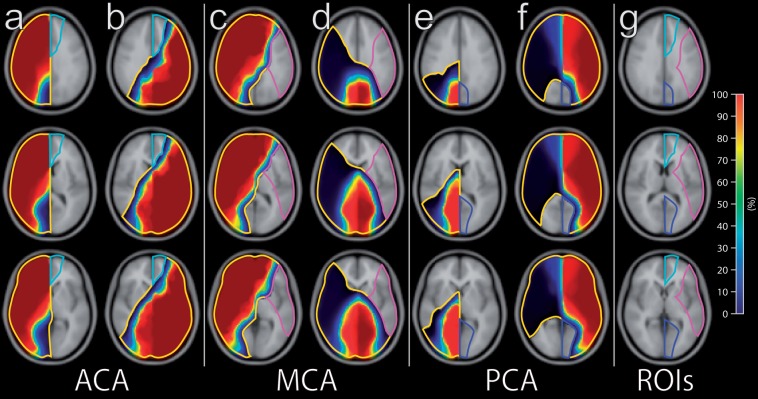
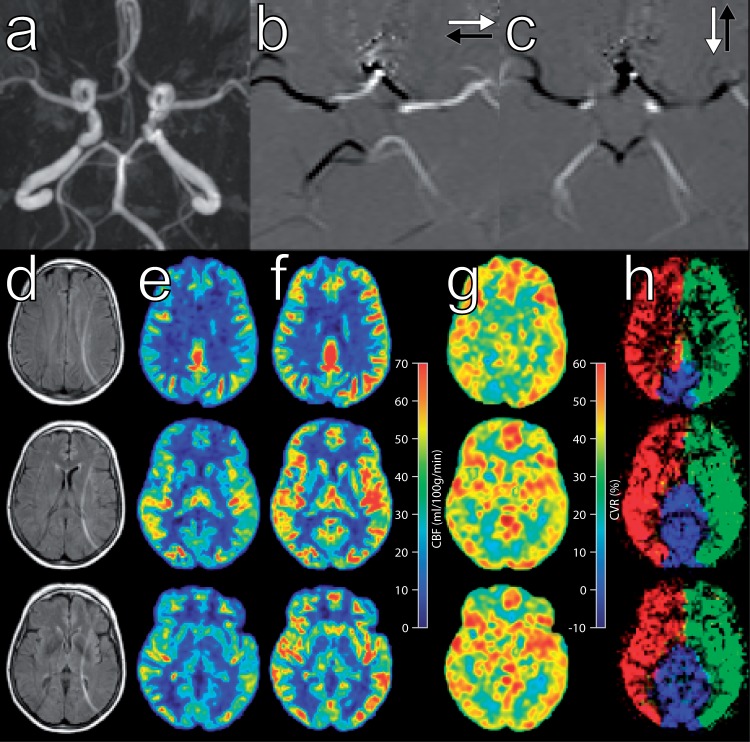
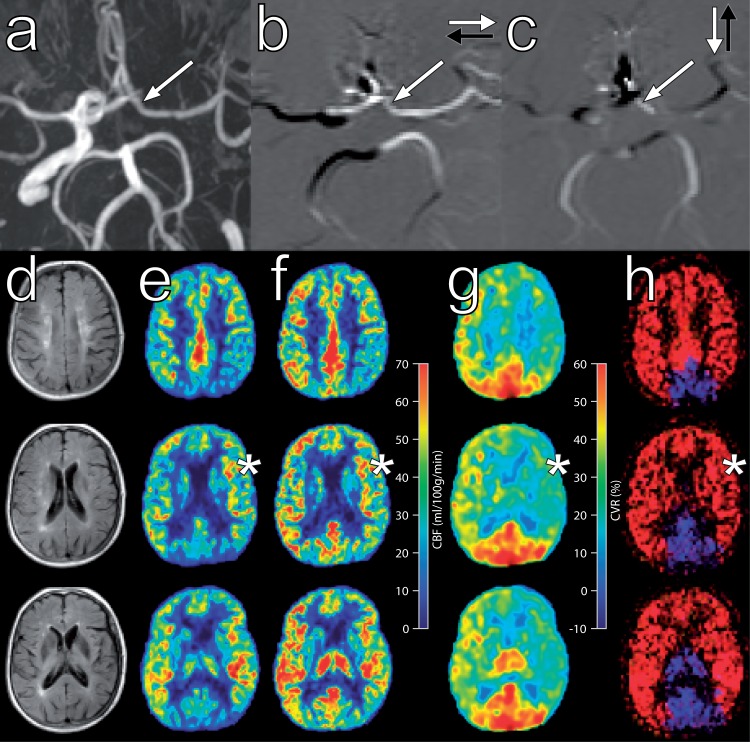
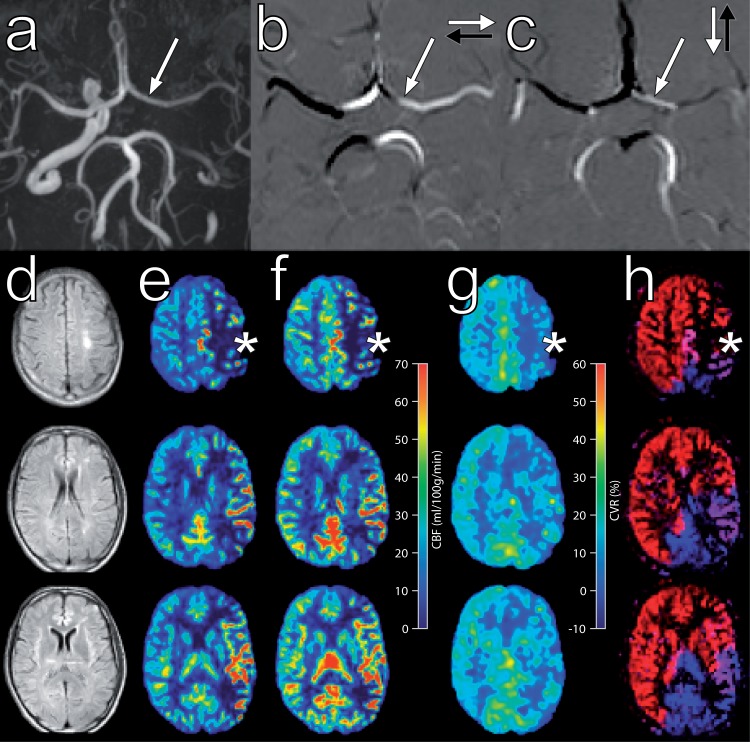
Collateral blood flow plays a pivotal role in steno-occlusive internal carotid artery (ICA) disease to prevent irreversible ischaemic damage. Our aim was to investigate the effect of carotid artery disease upon cerebral perfusion and cerebrovascular reactivity and whether haemodynamic impairment is influenced at brain tissue level by the existence of primary and/or secondary collateral. Eighty-eight patients with steno-occlusive ICA disease and 29 healthy controls underwent MR examination. The presence of collaterals was determined with time-of-flight, two-dimensional phase contrast MRA and territorial arterial spin labeling (ASL) imaging. Cerebral blood flow and cerebrovascular reactivity were assessed with ASL before and after acetazolamide. Cerebral haemodynamics were normal in asymptomatic ICA stenosis patients, as opposed to patients with ICA occlusion, in whom the haemodynamics in both hemispheres were compromised. Haemodynamic impairment in the affected brain region was always present in symptomatic patients. The degree of collateral blood flow was inversely correlated with haemodynamic impairment. Recruitment of secondary collaterals only occurred in symptomatic ICA occlusion patients. In conclusion, both CBF and cerebrovascular reactivity were found to be reduced in symptomatic patients with steno-occlusive ICA disease. The presence of collateral flow is associated with further haemodynamic impairment. Recruitment of secondary collaterals is associated with severe haemodynamic impairment.
Keywords: MRI; MRI angiography; Stroke; carotid artery; cerebral hemodynamics; perfusion-weighted MRI.
Figures
Similar articles
-
Intracerebral steal phenomenon in symptomatic carotid artery disease.J Neuroradiol. 2019 May;46(3):173-178. doi: 10.1016/j.neurad.2018.09.008. Epub 2018 Oct 30. J Neuroradiol. 2019. PMID: 30389512
-
Cerebrovascular reactivity within perfusion territories in patients with an internal carotid artery occlusion.J Neurol Neurosurg Psychiatry. 2011 Sep;82(9):1011-6. doi: 10.1136/jnnp.2010.233338. Epub 2011 Mar 8. J Neurol Neurosurg Psychiatry. 2011. PMID: 21386110
-
Spect measurements of regional cerebral perfusion and carbondioxide reactivity: correlation with cerebral collaterals in internal carotid artery occlusive disease.J Neurol. 2006 Oct;253(10):1285-91. doi: 10.1007/s00415-006-0192-1. Epub 2006 Oct 24. J Neurol. 2006. PMID: 17063318
-
Hemodynamics and oxygen extraction in chronic large artery steno-occlusive disease: Clinical applications for predicting stroke risk.J Cereb Blood Flow Metab. 2018 Sep;38(9):1584-1597. doi: 10.1177/0271678X17732884. Epub 2017 Sep 19. J Cereb Blood Flow Metab. 2018. PMID: 28925313 Free PMC article. Review.
-
Revascularization of collaterals for hemodynamic stroke: insight on pathophysiology from the carotid occlusion surgery study.Stroke. 2012 Jul;43(7):1988-91. doi: 10.1161/STROKEAHA.112.650119. Epub 2012 May 29. Stroke. 2012. PMID: 22649169 Free PMC article. Review. No abstract available.
Cited by
-
Optimal timing for measuring cerebral blood flow after acetazolamide administration to detect preexisting cerebral hemodynamics and metabolism in patients with bilateral major cerebral artery steno-occlusive diseases: 15O positron emission tomography studies.Am J Nucl Med Mol Imaging. 2021 Dec 15;11(6):507-518. eCollection 2021. Am J Nucl Med Mol Imaging. 2021. PMID: 35003888 Free PMC article.
-
Internal carotid artery stenosis: hemodynamics in the ipsilateral ACA affects CT angiography manifestations.Front Neurosci. 2023 May 18;17:1129570. doi: 10.3389/fnins.2023.1129570. eCollection 2023. Front Neurosci. 2023. PMID: 37274206 Free PMC article.
-
Cerebral perfusion in patients with unilateral internal carotid artery occlusion by dual post-labeling delays arterial spin labeling imaging.World J Radiol. 2024 Sep 28;16(9):429-438. doi: 10.4329/wjr.v16.i9.429. World J Radiol. 2024. PMID: 39355390 Free PMC article.
-
Determination of the Unilaterally Damaged Region May Depend on the Asymmetry of Carotid Blood Flow Velocity in Hemiparkinsonian Monkey: A Pilot Study.Parkinsons Dis. 2022 Nov 9;2022:4382145. doi: 10.1155/2022/4382145. eCollection 2022. Parkinsons Dis. 2022. PMID: 36407681 Free PMC article.
-
Cerebral cortical microinfarcts in patients with internal carotid artery occlusion.J Cereb Blood Flow Metab. 2021 Oct;41(10):2690-2698. doi: 10.1177/0271678X211011288. Epub 2021 Apr 25. J Cereb Blood Flow Metab. 2021. PMID: 33899560 Free PMC article.
References
-
- Derdeyn CP, Grubb RLJ, Powers WJ. Cerebral hemodynamic impairment: methods of measurement and association with stroke risk. Neurology 1999; 53: 251–259. - PubMed
-
- Liebeskind DS. Collateral circulation. Stroke 2003; 34: 2279–2284. - PubMed
-
- Muller M, van der Graaf Y, Algra A, et al. Carotid atherosclerosis and progression of brain atrophy: the SMART-MR study. Ann Neurol 2011; 70: 237–244. - PubMed
-
- Hofmeijer J, Klijn CJM, Kappelle LJ, et al. Collateral circulation via the ophthalmic artery or leptomeningeal vessels is associated with impaired cerebral vasoreactivity in patients with symptomatic carotid artery occlusion. Cerebrovasc Dis 2002; 14: 22–26. - PubMed
-
- Barnett HJ, Taylor DW, Eliasziw M, et al. Benefit of carotid endarterectomy in patients with symptomatic moderate or severe stenosis. North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med 1998; 339: 1415–1425. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
