

Complete surgical resection improves outcome in INRG high-risk patients with localized neuroblastoma older than 18 months
- PMID: 28778185
- PMCID: PMC5543757
- DOI: 10.1186/s12885-017-3493-0
Complete surgical resection improves outcome in INRG high-risk patients with localized neuroblastoma older than 18 months
Abstract
Background: Although several studies have been conducted on the role of surgery in localized neuroblastoma, the impact of surgical timing and extent of primary tumor resection on outcome in high-risk patients remains controversial.
Methods: Patients from the German neuroblastoma trial NB97 with localized neuroblastoma INSS stage 1-3 age > 18 months were included for retrospective analysis. Imaging reports were reviewed by two independent physicians for Image Defined Risk Factors (IDRF). Operation notes and corresponding imaging reports were analyzed for surgical radicality. The extent of tumor resection was classified as complete resection (95-100%), gross total resection (90-95%), incomplete resection (50-90%), and biopsy (<50%) and correlated with local control rate and outcome. Patients were stratified according to the International Neuroblastoma Risk Group (INRG) staging system. Survival curves were estimated according to the method of Kaplan and Meier and compared by the log-rank test.
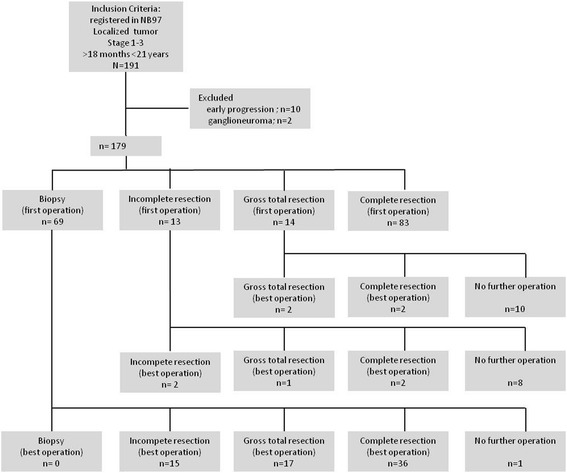
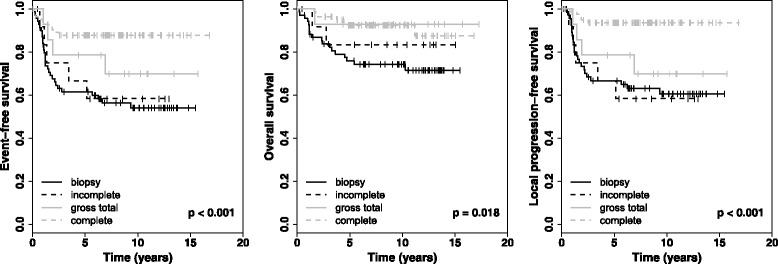
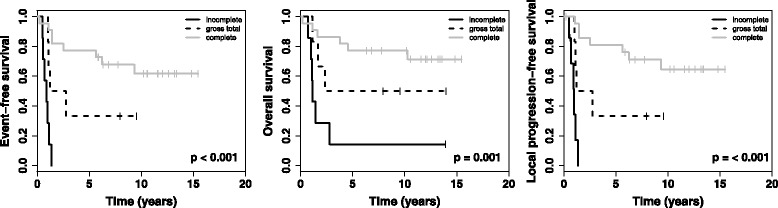
Results: A total of 179 patients were included in this study. 77 patients underwent more than one primary tumor operation. After best surgery, 68.7% of patients achieved complete resection of the primary tumor, 16.8% gross total resection, 14.0% incomplete surgery, and 0.5% biopsy only. The cumulative complication rate was 20.3% and the surgery associated mortality rate was 1.1%. Image defined risk factors (IDRF) predicted the extent of resection. Patients with complete resection had a better local-progression-free survival (LPFS), event-free survival (EFS) and OS (overall survival) than the other groups. Subgroup analyses showed better EFS, LPFS and OS for patients with complete resection in INRG high-risk patients. Multivariable analyses revealed resection (complete vs. other), and MYCN (non-amplified vs. amplified) as independent prognostic factors for EFS, LPFS and OS.
Conclusions: In patients with localized neuroblastoma age 18 months or older, especially in INRG high-risk patients harboring MYCN amplification, extended surgery of the primary tumor site improved local control rate and survival with an acceptable risk of complications.
Keywords: High-risk neuroblastoma; Localized neuroblastoma; Neuroblastoma surgery; Surgical oncology.
Conflict of interest statement
Competing interests
The authors declare that they have no competing interests.
Ethics approval and consent to participate
The trial was approved by Ethics Committee of the University Hospital of Cologne (no. 9764). Written informed consent was obtained from patients or their guardians for participation in the study design, data collection and treatment (Registration number: NCT00017225,
Consent for publication
Not applicable.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- De Bernardi B, Mosseri V, Rubie H, Castel V, Foot A, Ladenstein R, Laureys G, Beck-Popovic M, de Lacerda AF, Pearson AD, et al. Treatment of localised resectable neuroblastoma. Results of the LNESG1 study by the SIOP Europe neuroblastoma group. Br J Cancer. 2008;99(7):1027–1033. doi: 10.1038/sj.bjc.6604640. - DOI - PMC - PubMed
-
- Alvarado CS, London WB, Look AT, Brodeur GM, Altmiller DH, Thorner PS, Joshi VV, Rowe ST, Nash MB, Smith EI, et al. Natural history and biology of stage a neuroblastoma: a pediatric oncology group study. J Pediatr Hematol Oncol. 2000;22(3):197–205. doi: 10.1097/00043426-200005000-00003. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
