

Epidemiology of AKI: Utilizing Large Databases to Determine the Burden of AKI
- PMID: 28778358
- PMCID: PMC5648688
- DOI: 10.1053/j.ackd.2017.05.001
Epidemiology of AKI: Utilizing Large Databases to Determine the Burden of AKI
Abstract
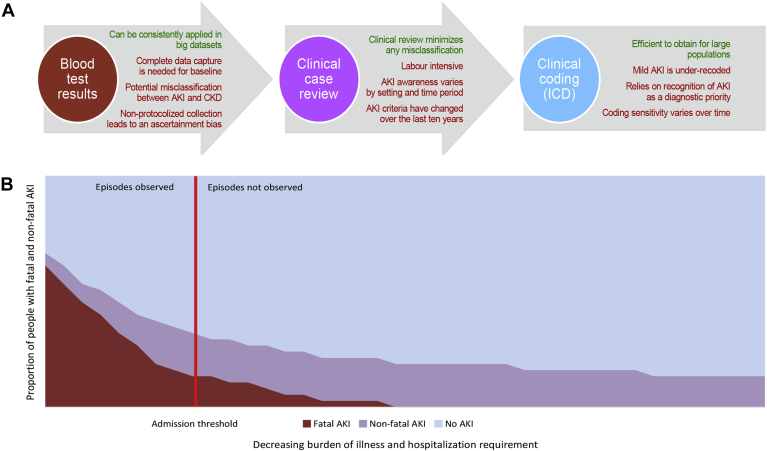
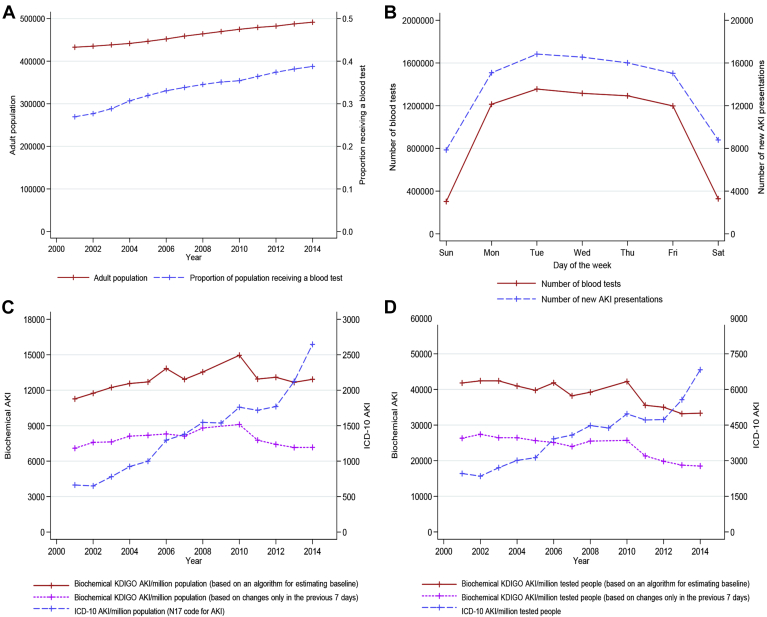
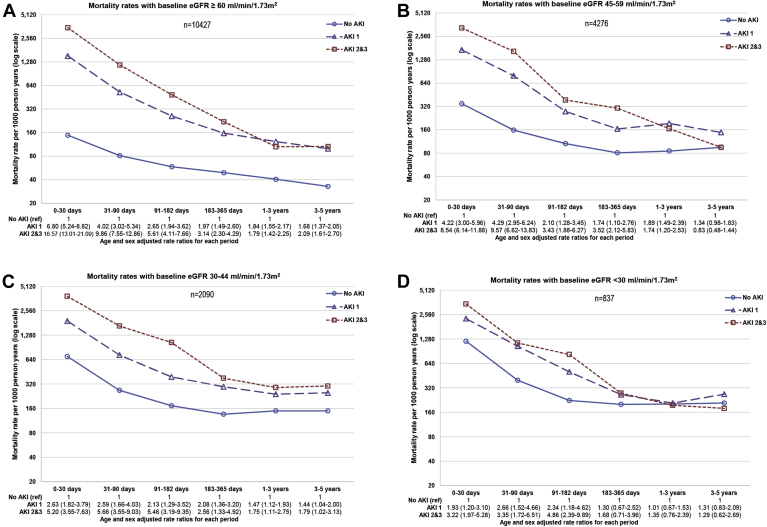
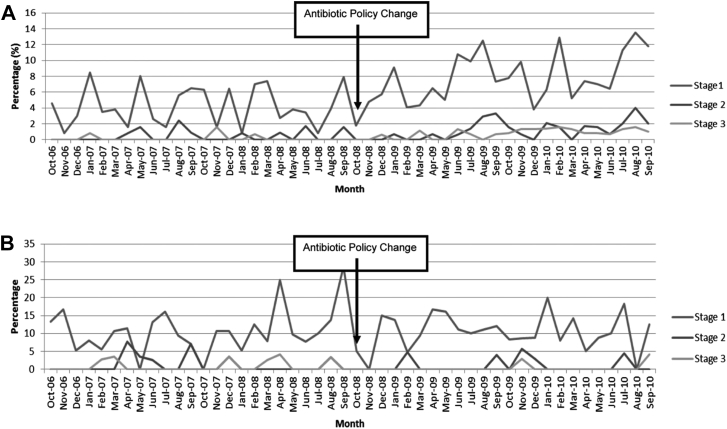
Large observational databases linking kidney function and other routine patient health data are increasingly being used to study acute kidney injury (AKI). Routine health care data show an apparent rise in the incidence of population AKI and an increase in acute dialysis. Studies also report an excess in mortality and adverse renal outcomes after AKI, although with variation depending on AKI severity, baseline, definition of renal recovery, and the time point during follow-up. However, differences in data capture, AKI awareness, monitoring, recognition, and clinical practice make comparisons between health care settings and periods difficult. In this review, we describe the growing role of large databases in determining the incidence and prognosis of AKI and evaluating initiatives to improve the quality of care in AKI. Using examples, we illustrate this use of routinely collected health data and discuss the strengths, limitations, and implications for researchers and clinicians.
Keywords: Acute kidney injury; Big-data; Incidence; Prognosis; Quality improvement.
Copyright © 2017 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Feynman R. What is science? Phys Teach. 1969;7(6):313–320.
-
- Lilienfeld D. Celebration: William Farr (1807–1883)—an appreciation on the 200th anniversary of his birth. Int J Epidemiol. 2007;36(5):985–987.
-
- Coorevits P., Sundgren M., Klein G.O. Electronic health records: new opportunities for clinical research. J Intern Med. 2013;274(6):547–560. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
