

Pragmatic Randomized, Controlled Trial of Patient Navigators and Enhanced Personal Health Records in CKD
- PMID: 28778854
- PMCID: PMC5586570
- DOI: 10.2215/CJN.02100217
Pragmatic Randomized, Controlled Trial of Patient Navigators and Enhanced Personal Health Records in CKD
Abstract
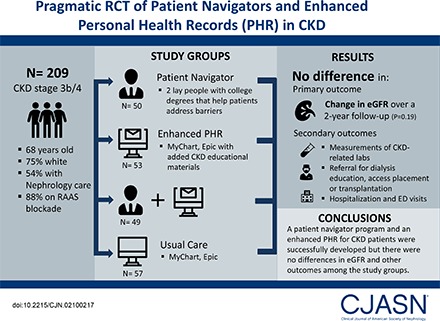
Background and objectives: Patient navigators and enhanced personal health records improve the quality of health care delivered in other disease states. We aimed to develop a navigator program for patients with CKD and an electronic health record-based enhanced personal health record to disseminate CKD stage-specific goals of care and education. We also conducted a pragmatic randomized clinical trial to compare the effect of a navigator program for patients with CKD with enhanced personal health record and compare their combination compared with usual care among patients with CKD stage 3b/4.
Design, setting, participants, & measurements: Two hundred and nine patients from six outpatient clinics (in both primary care and nephrology settings) were randomized in a 2×2 factorial design into four-study groups: (1) enhanced personal health record only, (2) patient navigator only, (3) both, and (4) usual care (control) group. Primary outcome measure was the change in eGFR over a 2-year follow-up period. Secondary outcome measures included acquisition of appropriate CKD-related laboratory measures, specialty referrals, and hospitalization rates.
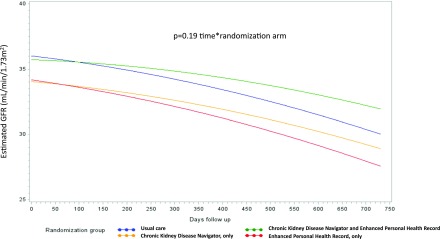
Results: Median age of the study population was 68 years old, and 75% were white. At study entry, 54% of patients were followed by nephrologists, and 88% were on renin-angiotensin system blockers. After a 2-year follow-up, rate of decline in eGFR was similar across the four groups (P=0.19). Measurements of CKD-related laboratory parameters were not significantly different among the groups. Furthermore, referral for dialysis education and vascular access placement, emergency room visits, and hospitalization rates were not statistically significant different between the groups.
Conclusions: We successfully developed a patient navigator program and an enhanced personal health record for the CKD population. However, there were no differences in eGFR decline and other outcomes among the study groups. Larger and long-term studies along with cost-effectiveness analyses are needed to evaluate the role of patient navigators and patient education through an enhanced personal health record in those with CKD.
Keywords: Aged; Ambulatory Care Facilities; Cost-Benefit Analysis; Electronic Health Records; Emergency Service, Hospital; Follow-Up Studies; Health Records, Personal; Humans; Nephrologists; Outcome Assessment (Health Care); Patient Care Planning; Patient Navigation; Primary Health Care; Referral and Consultation; Renal Insufficiency, Chronic; Renin-Angiotensin System; hospitalization; kidney disease; navigator; nephrology; personal health record; renal dialysis.
Copyright © 2017 by the American Society of Nephrology.
Figures

Comment in
-
The Times, They Are A-Changin: Innovations in Health Care Delivery To Reduce CKD Progression.Clin J Am Soc Nephrol. 2017 Sep 7;12(9):1375-1376. doi: 10.2215/CJN.07410717. Epub 2017 Aug 4. Clin J Am Soc Nephrol. 2017. PMID: 28778853 Free PMC article. No abstract available.
References
-
- Murphy D, McCulloch CE, Lin F, Banerjee T, Bragg-Gresham JL, Eberhardt MS, Morgenstern H, Pavkov ME, Saran R, Powe NR, Hsu CY; Centers for Disease Control and Prevention Chronic Kidney Disease Surveillance Team : Trends in prevalence of chronic kidney disease in the united states. Ann Intern Med 165: 473–481, 2016 - PMC - PubMed
-
- United States Renal Data System. 2016 USRDS Annual Data Report: Expenditures for Persons with CKD. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2016
-
- Kuhn L, Reeves K, Taylor Y, Tapp H, McWilliams A, Gunter A, Cleveland J, Dulin M: Planning for action: The impact of an asthma action plan decision support tool integrated into an electronic health record (EHR) at a large health care system. J Am Board Fam Med 28: 382–393, 2015 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
