

Advanced Roux-en-Y hepaticojejunostomy with magnetic compressive anastomats in obstructive jaundice dog models
- PMID: 28779259
- PMCID: PMC5772124
- DOI: 10.1007/s00464-017-5740-5
Advanced Roux-en-Y hepaticojejunostomy with magnetic compressive anastomats in obstructive jaundice dog models
Abstract
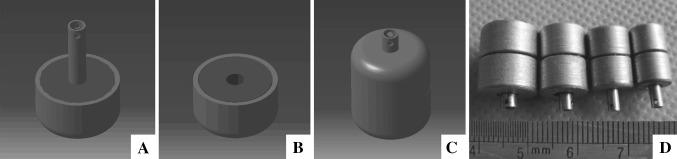
Background: Although commonly used procedure, Roux-en-Y hepaticojejunostomy (RYHJ) remains to be complicated, time consuming, and has a relatively poor prognosis. We designed the magnetic compressive anastomats (MCAs) to perform RYHJ more efficiently and safely.
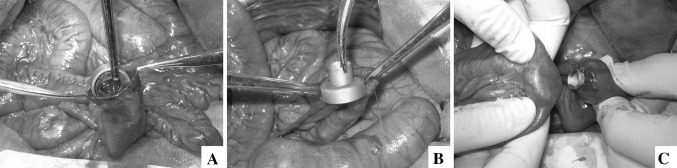
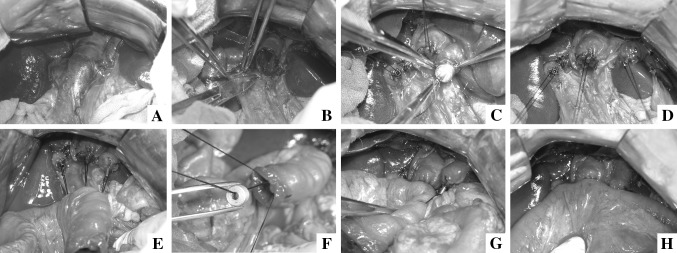
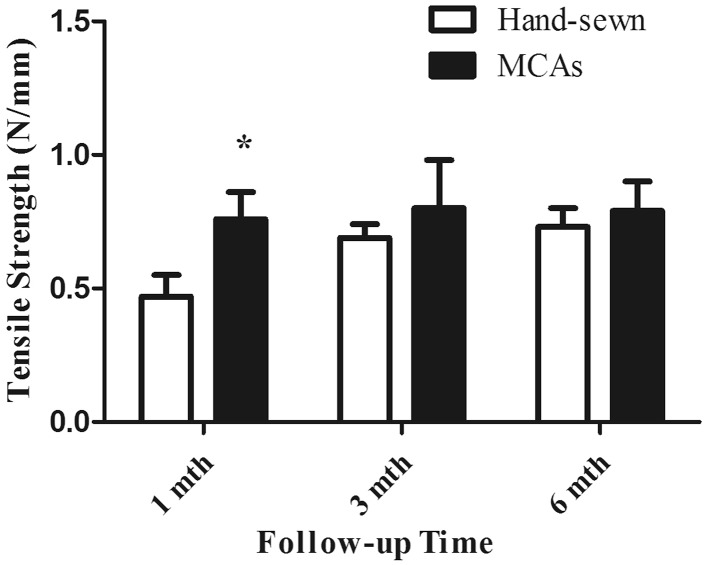
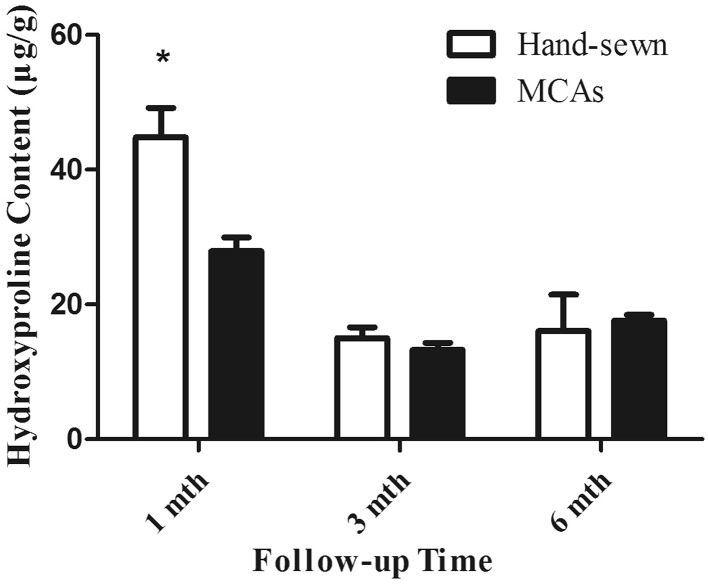
Materials and methods: 36 dogs were divided into two groups randomly. After obstructive jaundice model construction, RYHJ was performed with MCAs in study group or by hand-sewn in control group. Both groups were followed for 1, 3, and 6 months after RYHJ. The liver function and postoperative complications were recorded throughout the follow-up. At the end of each time point, dogs were sent for magnetic resonance imaging (MRI) and sacrificed. Anastomotic samples were taken for anastomotic narrowing rate calculation, histological analyses, tensile strength testing, and hydroxyproline content testing.
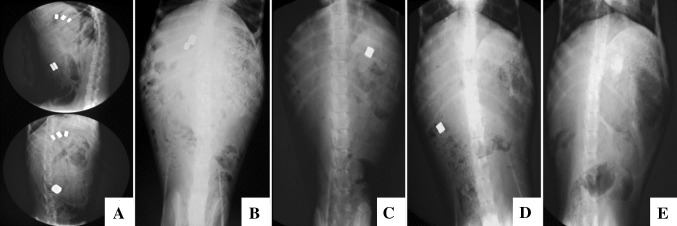
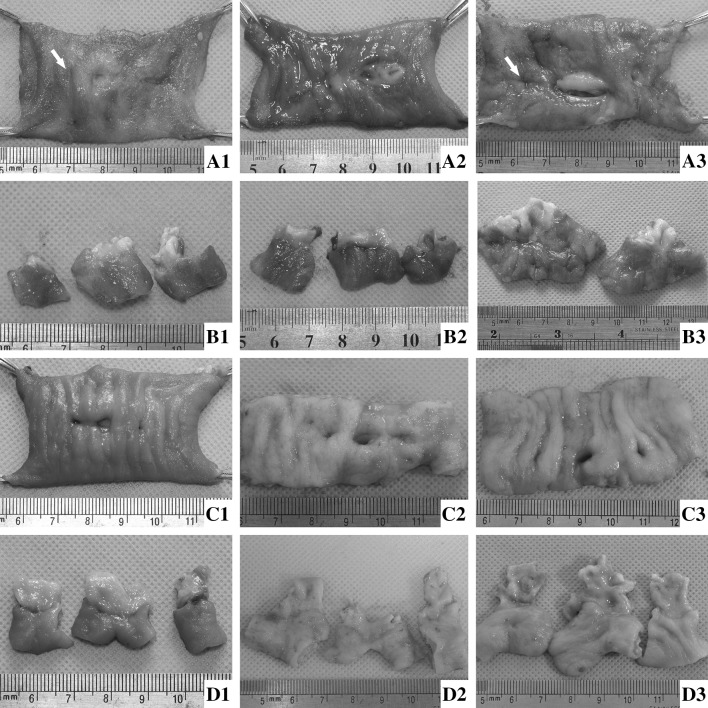
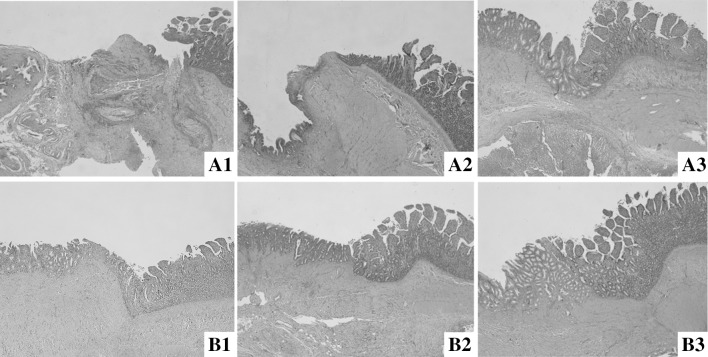
Results: The anastomotic construction times were 44.20 ± 23.02 min in study group, compared of 60.53 ± 11.89 min in control group (p < 0.05). The liver function recovered gradually after RYHJ in both groups (p > 0.05). All anastomats were expelled out of the body in 8.81 ± 2.01 days. The gross incidence of morbidity and mortality was 33.3% (6/18) and 16.7% (3/18) in study group compared with 38.9% (7/18) and 22.2% (4/18) in control group (p > 0.05), and there is no single case of anastomotic-specific complications happened in study group. The narrowing rates of anastomosis were 14.6, 18.5, and 18.7% in study group compared with 35.4, 36.9, and 34% in control group at 1st, 3rd, and 6th month after RYHJ (p < 0.05). In study group, preciser alignment of tissue layers and milder inflammatory reaction contributed to the fast and better wound healing process.
Conclusion: Perform RYHJ with MCAs is safer, more efficient than by hand-sewn method in obstructive jaundice dog models.
Keywords: Anastomat; Bilioenteric anastomosis; Hepaticojejunostomy; Magnetic compression anastomosis; Obstructive jaundice; Sutureless; Wound healing.
Conflict of interest statement
During the conduct of this work, Chao Fan, Hongke Zhang, Xiao-peng Yan, Jia Ma, ChunBao Wang, and Yi Lv have no conflicts of interest to disclose.
Figures
References
-
- Antolovic D, Koch M, Galindo L, Wolff S, Music E, Kienle P, Schemmer P, Friess H, Schmidt J, Buchler MW, Weitz J. Hepaticojejunostomy—analysis of risk factors for postoperative bile leaks and surgical complications. J Gastrointest Surg. 2007;11:555–561. doi: 10.1007/s11605-007-0166-3. - DOI - PubMed
-
- Obora Y, Tamaki N, Matsumoto S. Non-suture micro-vascular anastomosis using magnet rings—preliminary-report. Surg Neurol. 1978;9:117–120. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
