

Reduced Antiplatelet Effect of Aspirin Does Not Predict Cardiovascular Events in Patients With Stable Coronary Artery Disease
- PMID: 28780510
- PMCID: PMC5586446
- DOI: 10.1161/JAHA.117.006050
Reduced Antiplatelet Effect of Aspirin Does Not Predict Cardiovascular Events in Patients With Stable Coronary Artery Disease
Abstract
Background: Increased platelet aggregation during antiplatelet therapy may predict cardiovascular events in patients with coronary artery disease. The majority of these patients receive aspirin monotherapy. We aimed to investigate whether high platelet-aggregation levels predict cardiovascular events in stable coronary artery disease patients treated with aspirin.
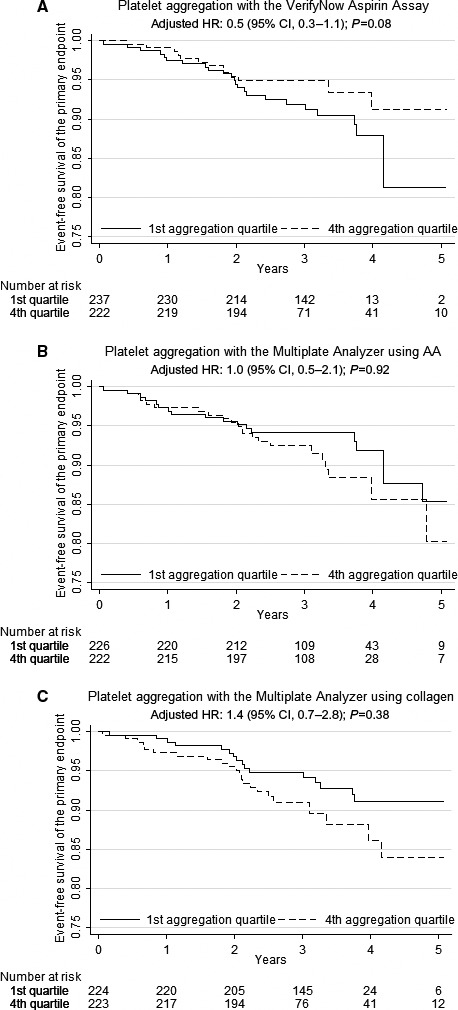
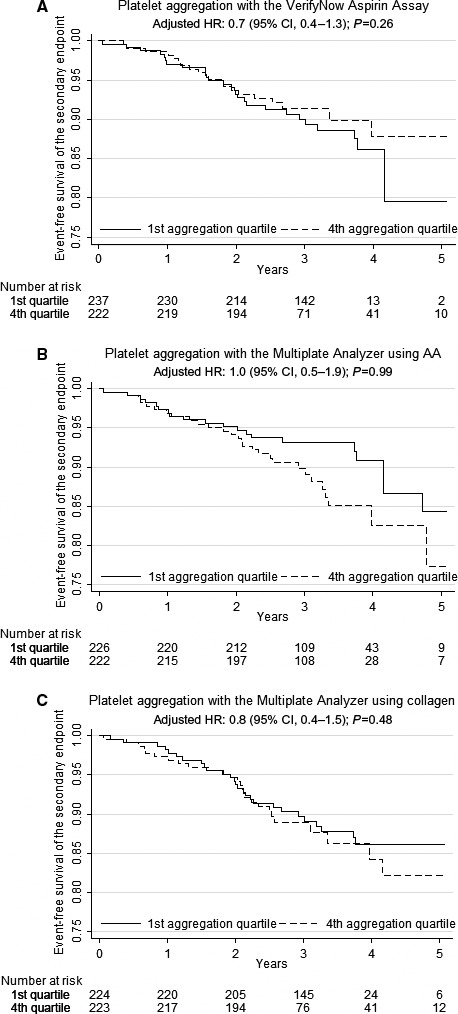
Methods and results: We included 900 stable coronary artery disease patients with either previous myocardial infarction, type 2 diabetes mellitus, or both. All patients received single antithrombotic therapy with 75 mg aspirin daily. Platelet aggregation was evaluated 1 hour after aspirin intake using the VerifyNow Aspirin Assay (Accriva Diagnostics) and Multiplate Analyzer (Roche; agonists: arachidonic acid and collagen). Adherence to aspirin was confirmed by serum thromboxane B2. The primary end point was the composite of nonfatal myocardial infarction, ischemic stroke, and cardiovascular death. At 3-year follow-up, 78 primary end points were registered. The primary end point did not occur more frequently in patients with high platelet-aggregation levels (first versus fourth quartile) assessed by VerifyNow (hazard ratio: 0.5 [95% CI, 0.3-1.1], P=0.08) or Multiplate using arachidonic acid (hazard ratio: 1.0 [95% CI, 0.5-2.1], P=0.92) or collagen (hazard ratio: 1.4 [95% CI, 0.7-2.8], P=0.38). Similar results were found for the composite secondary end point (nonfatal myocardial infarction, ischemic stroke, stent thrombosis, and all-cause death) and the single end points. Thromboxane B2 levels did not predict any end points. Renal insufficiency was the only clinical risk factor predicting the primary and secondary end points.
Conclusions: This study is the largest to investigate platelet aggregation in stable coronary artery disease patients receiving aspirin as single antithrombotic therapy. We found that high platelet-aggregation levels did not predict cardiovascular events.
Keywords: antiplatelet drug resistance; aspirin; coronary artery disease; prognosis.
© 2017 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
Similar articles
-
Antiplatelet effect of aspirin in patients with coronary artery disease.Dan Med J. 2012 Sep;59(9):B4506. Dan Med J. 2012. PMID: 22951204 Review.
-
Determinants of reduced antiplatelet effect of aspirin in patients with stable coronary artery disease.PLoS One. 2015 May 18;10(5):e0126767. doi: 10.1371/journal.pone.0126767. eCollection 2015. PLoS One. 2015. PMID: 25993271 Free PMC article.
-
Platelet reactivity and cardiovascular events after percutaneous coronary intervention in patients with stable coronary artery disease: the Stent Thrombosis In Belgium (STIB) trial.EuroIntervention. 2014 Jun;10(2):204-11. doi: 10.4244/EIJV10I2A34. EuroIntervention. 2014. PMID: 24952058 Clinical Trial.
-
Aspirin in coronary artery disease: an appraisal of functions and limitations.Dan Med J. 2015 Apr;62(4):B5011. Dan Med J. 2015. PMID: 25872543 Review.
-
Platelet Reactivity and Clinical Outcomes After Coronary Artery Implantation of Drug-Eluting Stents in Subjects With Peripheral Arterial Disease: Analysis From the ADAPT-DES Study (Assessment of Dual Antiplatelet Therapy With Drug-Eluting Stents).Circ Cardiovasc Interv. 2017 Mar;10(3):e004904. doi: 10.1161/CIRCINTERVENTIONS.116.004904. Circ Cardiovasc Interv. 2017. PMID: 28288963
Cited by
-
Aspirin Versus Clopidogrel Monotherapy for the Treatment of Patients with Stable Coronary Artery Disease: A Systematic Review and Meta-Analysis.Adv Ther. 2019 Aug;36(8):2062-2071. doi: 10.1007/s12325-019-01004-6. Epub 2019 Jun 1. Adv Ther. 2019. PMID: 31154631 Free PMC article.
-
Effects of Ramadan fasting on aspirin resistance in type 2 diabetic patients.PLoS One. 2018 Mar 12;13(3):e0192590. doi: 10.1371/journal.pone.0192590. eCollection 2018. PLoS One. 2018. PMID: 29529091 Free PMC article. Clinical Trial.
-
Factors Associated with Aspirin Resistance in Hong Kong Chinese Patients with Stable Coronary Heart Disease Using the Multiplate® Analyzer and Serum Thromboxane B2.Pharmaceutics. 2022 Oct 1;14(10):2099. doi: 10.3390/pharmaceutics14102099. Pharmaceutics. 2022. PMID: 36297534 Free PMC article.
-
Early assessment of the pharmacokinetic and pharmacodynamic effects following acetylsalicylic acid loading: toward a definition for acute therapeutic response.J Thromb Thrombolysis. 2024 Jan;57(1):21-28. doi: 10.1007/s11239-023-02914-7. Epub 2023 Dec 8. J Thromb Thrombolysis. 2024. PMID: 38066385 Free PMC article.
-
Potentiation of thrombus instability: a contributory mechanism to the effectiveness of antithrombotic medications.J Thromb Thrombolysis. 2018 May;45(4):593-602. doi: 10.1007/s11239-018-1641-2. J Thromb Thrombolysis. 2018. PMID: 29550950 Free PMC article. Review.
References
-
- Juul‐Moller S, Edvardsson N, Jahnmatz B, Rosen A, Sorensen S, Omblus R. Double‐blind trial of aspirin in primary prevention of myocardial infarction in patients with stable chronic angina pectoris. The Swedish Angina Pectoris Aspirin Trial (SAPAT) Group. Lancet. 1992;340:1421–1425. - PubMed
-
- Baigent C, Blackwell L, Collins R, Emberson J, Godwin J, Peto R, Buring J, Hennekens C, Kearney P, Meade T, Patrono C, Roncaglioni MC, Zanchetti A. Aspirin in the primary and secondary prevention of vascular disease: collaborative meta‐analysis of individual participant data from randomised trials. Lancet. 2009;373:1849–1860. - PMC - PubMed
-
- Santilli F, Rocca B, De Cristofaro R, Lattanzio S, Pietrangelo L, Habib A, Pettinella C, Recchiuti A, Ferrante E, Ciabattoni G, Davi G, Patrono C. Platelet cyclooxygenase inhibition by low‐dose aspirin is not reflected consistently by platelet function assays: implications for aspirin “resistance”. J Am Coll Cardiol. 2009;53:667–677. - PubMed
-
- Siller‐Matula JM, Christ G, Lang IM, Delle‐Karth G, Huber K, Jilma B. Multiple electrode aggregometry predicts stent thrombosis better than the vasodilator‐stimulated phosphoprotein phosphorylation assay. J Thromb Haemost. 2010;8:351–359. - PubMed
-
- Breet NJ, van Werkum JW, Bouman HJ, Kelder JC, Ruven HJ, Bal ET, Deneer VH, Harmsze AM, van der Heyden JA, Rensing BJ, Suttorp MJ, Hackeng CM, ten Berg JM. Comparison of platelet function tests in predicting clinical outcome in patients undergoing coronary stent implantation. JAMA. 2010;303:754–762. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
