

FRAX- vs. T-score-based intervention thresholds for osteoporosis
- PMID: 28782072
- PMCID: PMC5881885
- DOI: 10.1007/s00198-017-4160-7
FRAX- vs. T-score-based intervention thresholds for osteoporosis
Abstract
Many current guidelines for the assessment of osteoporosis, including those in Kuwait, initiate fracture risk assessment in men and women using BMD T-score thresholds. We compared the Kuwaiti guidelines with FRAX-based age-dependent intervention thresholds equivalent to that in women with a prior fragility fracture. FRAX-based intervention thresholds identified women at higher fracture probability than fixed T-score thresholds, particularly in the elderly.
Purpose: A FRAX® model been recently calibrated for Kuwait, but guidance is needed on how to utilise fracture probabilities in the assessment and treatment of patients.
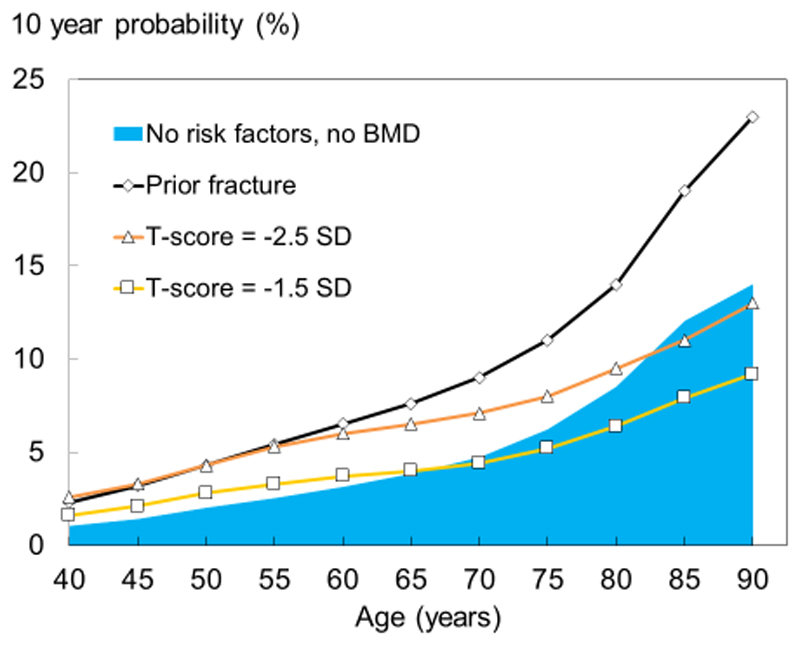
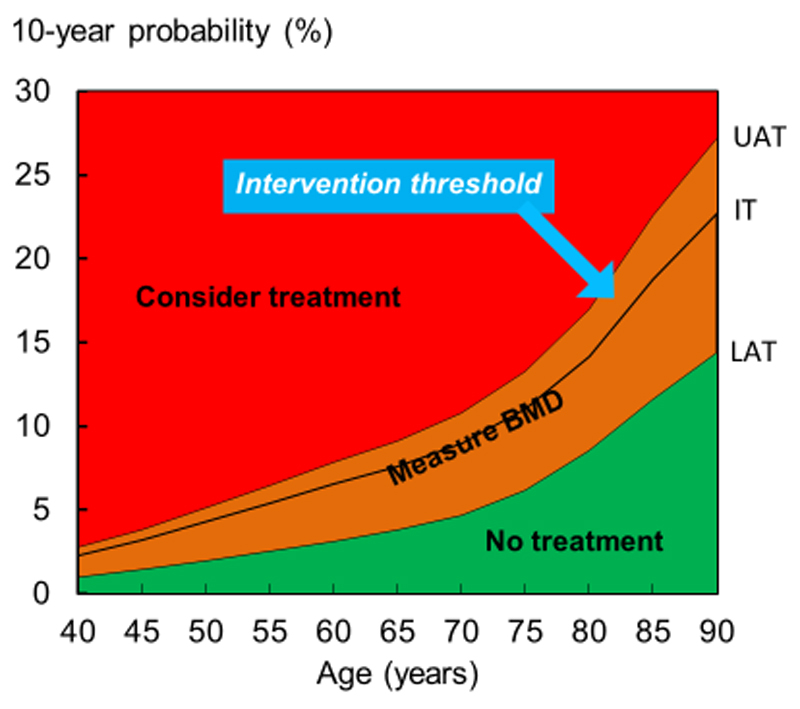
Methods: We compared age-specific fracture probabilities, equivalent to women with no clinical risk factors and a prior fragility fracture (without BMD), with the age-specific fracture probabilities associated with femoral neck T-scores of -2.5 and -1.5 SD, in line with current guidelines in Kuwait. Upper and lower assessment thresholds for BMD testing were additionally explored using FRAX.
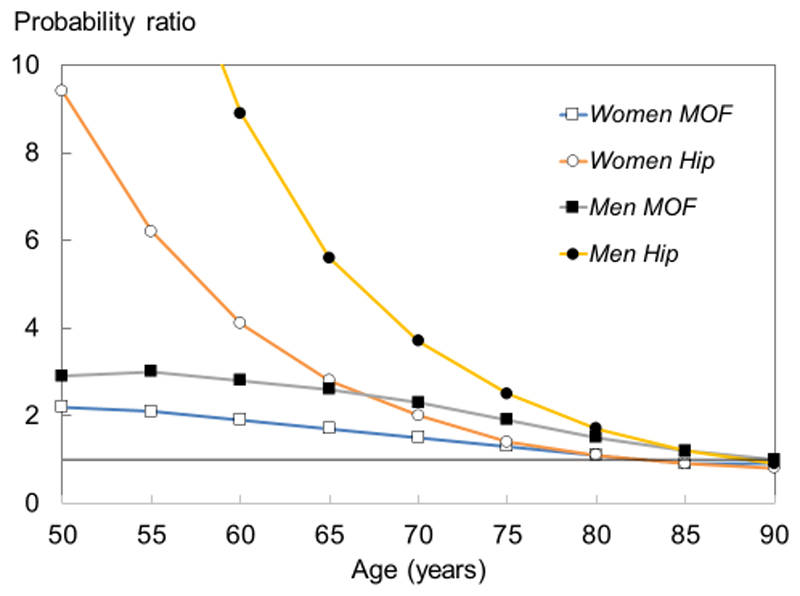
Results: When a BMD T-score of -2.5 SD was used as an intervention threshold, FRAX probabilities of a major osteoporotic fracture in women aged 50 years were approximately twofold higher than those in women of the same age but with an average BMD. The increase in risk associated with the BMD threshold decreased progressively with age such that, at the age of 83 years or more, a T-score of -2.5 SD was associated with a lower probability of fracture than that of the age-matched general population with no clinical risk factors. The same phenomenon was observed from the age of 66 years at a T-score of -1.5 SD. A FRAX-based intervention threshold, defined as the 10-year probability of a major osteoporotic fracture in a woman of average BMI with a previous fracture, rose with age from 4.3% at the age of 50 years to 23%, at the age of 90 years, and identified women at increased risk at all ages. Qualitatively comparable findings were observed in the case of hip fracture probability and in men.
Conclusion: Intervention thresholds based on BMD alone do not optimally target women at higher fracture risk than those on age-matched individuals without clinical risk factors, particularly in the elderly. In contrast, intervention thresholds based on fracture probabilities equivalent to a 'fracture threshold' consistently target women at higher fracture risk, irrespective of age.
Keywords: FRAX; Fracture probability; Intervention threshold; Kuwait; Osteoporosis.
Conflict of interest statement
Professor Kanis led the team that developed FRAX as director of the then WHO Collaborating Centre for Metabolic Bone Diseases; he has no financial interest in FRAX. Professors McCloskey, Oden, Harvey and Dr Johansson are members of the FRAX team. Professors Harvey, Kanis and McCloskey are members of the Expert Advisory Group of the National Osteoporosis Guideline Group, UK.
Figures
References
-
- Kanis JA, Melton LJ, Christiansen C, Johnston C, Khaltaev N. The diagnosis of osteoporosis. J Bone Miner Res. 1994;9:1137–1141. - PubMed
-
- Kanis JA, McCloskey EV, Johansson H, Oden A, Melton LJ, 3rd, Khaltaev N. A reference standard for the description of osteoporosis. Bone. 2008;42:467–475. - PubMed
-
- World Health Organisation. WHO Technical Report Series 843. WHO; Geneva: 1994. Assessment of fracture risk and its application to screening for postmenopausal osteoporosis. - PubMed
-
- Kanis JA, Johnell O, De Laet C, et al. A meta-analysis of previous fracture and subsequent fracture risk. Bone. 2004a;35:375–382. - PubMed
-
- Kanis JA, Johansson H, Oden A, et al. A family history of fracture and fracture risk: a meta-analysis. Bone. 2004;35:1029–1037. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
