

A comparison of early versus late initiation of renal replacement therapy for acute kidney injury in critically ill patients: an updated systematic review and meta-analysis of randomized controlled trials
- PMID: 28784106
- PMCID: PMC5547509
- DOI: 10.1186/s12882-017-0667-6
A comparison of early versus late initiation of renal replacement therapy for acute kidney injury in critically ill patients: an updated systematic review and meta-analysis of randomized controlled trials
Abstract
Background: To investigate the impact of timing the initiation of renal replacement therapy (RRT) on clinical outcomes in critically ill patients with acute kidney injury (AKI), focusing on the randomized controlled trials (RCTs) in this field.
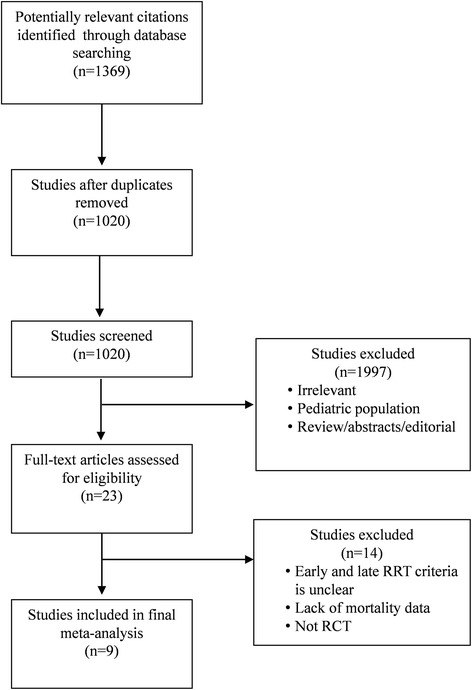
Methods: The PubMed, EMBASE and Cochrane databases were searched between January 1, 1985, and June 30, 2016, to identify randomized trials that assessed the timing of initiation of RRT in patients with AKI.
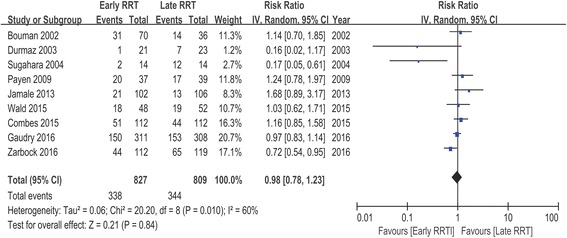
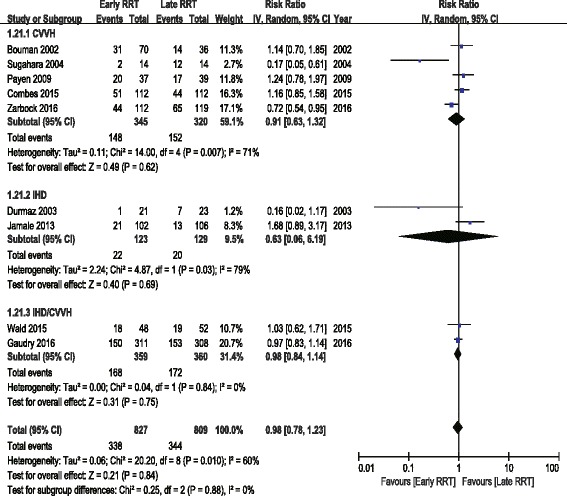
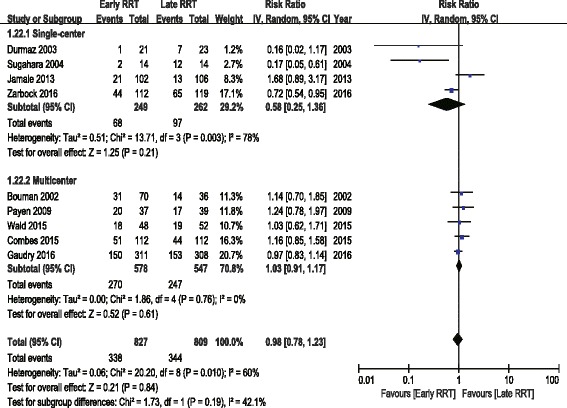
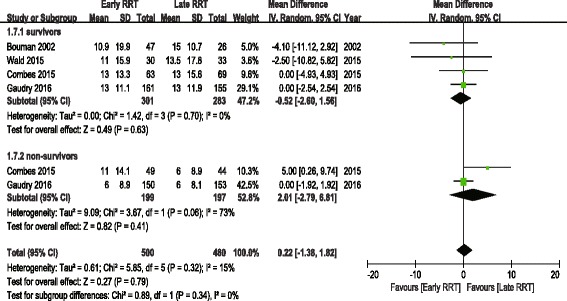
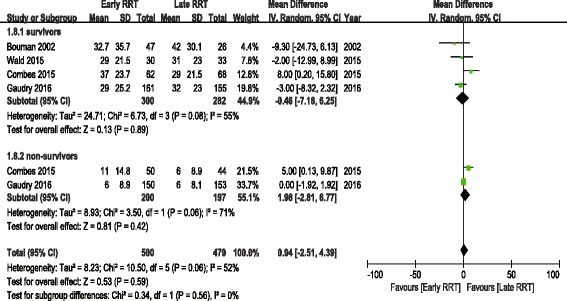
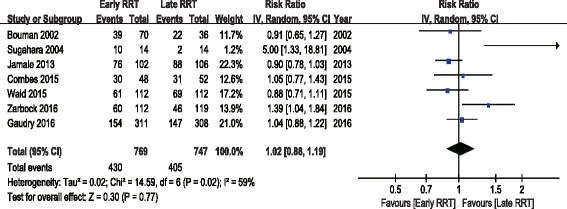
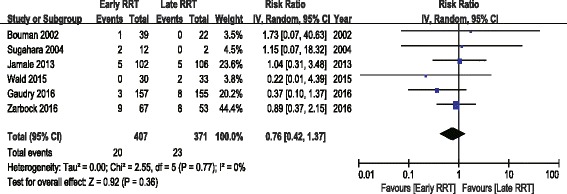
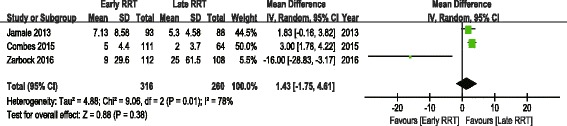
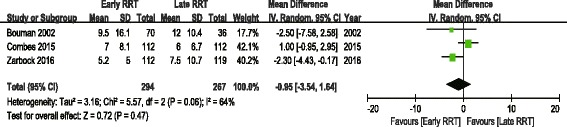
Results: Nine RCTs, with a total of 1636 patients, were enrolled in this meta-analysis. A pooled analysis of the studies indicated no mortality benefit with "early" RRT, with an RR of 0.98 (95% CI 0.78 to 1.23, P = 0.84). There was no significant difference in intensive care unit (ICU) length of stay (LOS) or hospital LOS between the early and late RRT groups for survivors or nonsurvivors. Pooled analysis also demonstrated no significant change in renal function recovery (RR 1.02, 95% CI 0.88 to 1.19, I2 = 59%), RRT dependence (RR 0.76, 95% CI 0.42 to 1.37, I2 = 0%), duration of RRT (Mean difference 1.43, 95% CI -1.75 to 4.61, I2 = 78%), renal recovery time (Mean difference 0.73, 95% CI -2.09 to 3.56, I2 = 70%) or mechanical ventilation time (Mean difference - 0.95, 95% CI -3.54 to 1.64, I2 = 64%) between the early and late RRT groups. We found no significant differences in complications between the groups.
Conclusions: Our meta-analysis revealed that the "early" initiation of RRT in critically ill patients did not result in reduced mortality. Pooled analysis of secondary outcomes also showed no significant difference between the early and late RRT groups. More well-designed and large-scale trials are expected to confirm the result of this meta-analysis.
Keywords: Acute kidney injury; Renal replacement therapy; Timing.
Conflict of interest statement
Ethics approval and consent to participate
Ethics approval and consent waived. All the data presented in this review is from previously published studies.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Clec'h C, Gonzalez F, Lautrette A, Nguile-Makao M, Garrouste-Orgeas M, Jamali S, Golgran-Toledano D, Descorps-Declere A, Chemouni F, Hamidfar-Roy R, et al. Multiple-center evaluation of mortality associated with acute kidney injury in critically ill patients: a competing risks analysis. Crit Care. 2011;15(3):R128. doi: 10.1186/cc10241. - DOI - PMC - PubMed
-
- Vinsonneau C, Allain-Launay E, Blayau C, Darmon M, Ducheyron D, Gaillot T, Pm H, Javouhey E, Krummel T, Lahoche A, et al. Renal replacement therapy in adult and pediatric intensive care: recommendations by an expert panel from the French Intensive Care Society (Srlf) with the French society of anesthesia intensive care (Sfar) French group for pediatric intensive care emergencies (Gfrup) the French dialysis society (Sfd) Ann Intensive Care. 2015;5(1):58. doi: 10.1186/s13613-015-0093-5. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
