

Clinical practice variation and need for pediatric-specific treatment guidelines among rheumatologists caring for children with ANCA-associated vasculitis: an international clinician survey
- PMID: 28784150
- PMCID: PMC5545848
- DOI: 10.1186/s12969-017-0191-z
Clinical practice variation and need for pediatric-specific treatment guidelines among rheumatologists caring for children with ANCA-associated vasculitis: an international clinician survey
Abstract
Background: Because pediatric antineutrophil cytoplasmic antibody-associated vasculitis is rare, management generally relies on adult data. We assessed treatment practices, uptake of existing clinical assessment tools, and interest in pediatric treatment protocols among rheumatologists caring for children with granulomatosis with polyangiitis (GPA) and microscopic polyangiitis (MPA).
Methods: A needs-assessment survey developed by an international working group of pediatric rheumatologists and two nephrologists was circulated internationally. Data were summarized with descriptive statistics. Pearson's chi-square tests were used in inferential univariate analyses.
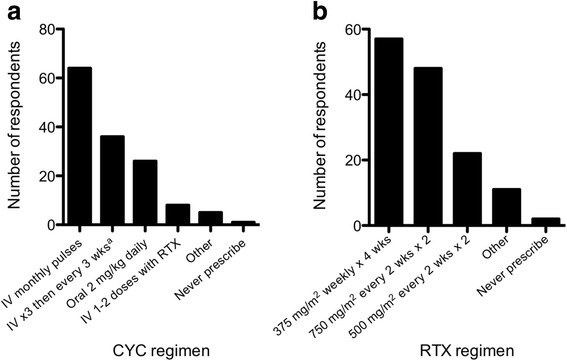
Results: The 209 respondents from 36 countries had collectively seen ~1600 children with GPA/MPA; 144 had seen more than two in the preceding 5 years. Standardized and validated clinical assessment tools to score disease severity, activity, and damage were used by 59, 63, and 36%, respectively; barriers to use included lack of knowledge and limited perceived utility. Therapy varied significantly: use of rituximab rather than cyclophosphamide was more common among respondents from the USA (OR = 2.7 [1.3-5.5], p = 0.0190, n = 139), those with >5 years of independent practice experience (OR = 3.8 [1.3-12.5], p = 0.0279, n = 137), and those who had seen >10 children with GPA/MPA in their careers (OR = 4.39 [2.1-9.1], p = 0.0011, n = 133). Respondents who had treated >10 patients were also more likely to continue maintenance therapy for at least 24 months (OR = 3.0 [1.4-6.4], p = 0.0161, n = 127). Ninety six percent of respondents believed in a need for pediatric-specific treatment guidelines; 46% supported adaptation of adult guidelines while 69% favoured guidelines providing a limited range of treatment options to allow comparison of effectiveness through a registry.
Conclusions: These data provide a rationale for developing pediatric-specific consensus treatment guidelines for GPA/MPA. While pediatric rheumatologist uptake of existing clinical tools has been limited, guideline uptake may be enhanced if outcomes of consensus-derived treatment options are evaluated within the framework of an international registry.
Keywords: Anti-neutrophil cytoplasmic antibody-associated vasculitis; Clinical practice guidelines; Disease classification; Granulomatosis with polyangiitis; Microscopic polyangiitis; Outcome assessment; Pediatric rheumatology; Physician practice patterns; Vasculitis treatment.
Conflict of interest statement
Ethics approval and consent to participate
The survey was conducted as a quality assurance initiative for PedVas, which was approved by the Children’s and Women’s Research Ethics Board of the University of British Columbia (H12-00894). Under Article 2.5 of the Tri Council Policy Statement, quality assurance/improvement activities are not subject to further institutional review.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Concordance between practice and published evidence in the management of ANCA-associated vasculitis in Japan: A cross-sectional web-questionnaire survey.Mod Rheumatol. 2023 Aug 25;33(5):990-997. doi: 10.1093/mr/roac118. Mod Rheumatol. 2023. PMID: 36181464
-
Insights from Portuguese Nephrologists and Rheumatologists Concerning the Treatment of ANCA Vasculitis.Acta Med Port. 2024 Nov 4;37(11):778-786. doi: 10.20344/amp.21635. Epub 2024 Nov 4. Acta Med Port. 2024. PMID: 39621592
-
Physicians' perceptions about antineutrophil cytoplasmic antibody-associated vasculitis: an online survey report in the time of the COVID-19 pandemic.Clin Rheumatol. 2023 Mar;42(3):831-837. doi: 10.1007/s10067-022-06452-0. Epub 2022 Nov 21. Clin Rheumatol. 2023. PMID: 36414862 Free PMC article.
-
Consensus Treatment Plans for Severe Pediatric Antineutrophil Cytoplasmic Antibody-Associated Vasculitis.Arthritis Care Res (Hoboken). 2022 Sep;74(9):1550-1558. doi: 10.1002/acr.24590. Epub 2022 Jun 1. Arthritis Care Res (Hoboken). 2022. PMID: 33675161 Review.
-
Biological drugs in ANCA-associated vasculitis.Int Immunopharmacol. 2015 Aug;27(2):209-12. doi: 10.1016/j.intimp.2015.04.023. Epub 2015 Apr 20. Int Immunopharmacol. 2015. PMID: 25907243 Review.
Cited by
-
The Association Between Age at Diagnosis and Disease Characteristics and Damage in Patients With ANCA-Associated Vasculitis.Arthritis Rheumatol. 2023 Dec;75(12):2216-2227. doi: 10.1002/art.42651. Epub 2023 Oct 5. Arthritis Rheumatol. 2023. PMID: 37433067 Free PMC article.
-
Hallmark trials in ANCA-associated vasculitis (AAV) for the pediatric rheumatologist.Pediatr Rheumatol Online J. 2019 Jun 26;17(1):31. doi: 10.1186/s12969-019-0343-4. Pediatr Rheumatol Online J. 2019. PMID: 31242923 Free PMC article. Review.
-
Childhood-Onset ANCA-Associated Vasculitis: From Genetic Studies to Advances in Pathogenesis, Classification and Novel Therapeutic Approaches.Int J Mol Sci. 2024 Dec 22;25(24):13704. doi: 10.3390/ijms252413704. Int J Mol Sci. 2024. PMID: 39769465 Free PMC article. Review.
-
S100A12 Serum Levels and PMN Counts Are Elevated in Childhood Systemic Vasculitides Especially Involving Proteinase 3 Specific Anti-neutrophil Cytoplasmic Antibodies.Front Pediatr. 2018 Nov 23;6:341. doi: 10.3389/fped.2018.00341. eCollection 2018. Front Pediatr. 2018. PMID: 30533405 Free PMC article.
-
[Diffuse alveolar hemorrhage in children].Zhongguo Dang Dai Er Ke Za Zhi. 2019 Sep;21(9):949-954. doi: 10.7499/j.issn.1008-8830.2019.09.020. Zhongguo Dang Dai Er Ke Za Zhi. 2019. PMID: 31506159 Free PMC article. Review. Chinese.
References
-
- Jennette JC, Falk RJ, Bacon PA, Basu N, Cid MC, Ferrario F, Flores-Suarez LF, Gross WL, Guillevin L, Hagen EC, et al. Revised international Chapel Hill consensus conference nomenclature of Vasculitides. Arthritis Rheum. 2012;2013(65):1–11. - PubMed
-
- Wilkinson NM, Page J, Uribe AG, Espinosa V, Cabral DA. Establishment of a pilot pediatric registry for chronic vasculitis is both essential and feasible: a childhood arthritis and rheumatology alliance (CARRA) survey. J Rheumatol. 2007;34:224–226. - PubMed
-
- Cabral D, Benseler S, Foell D, Hancock RE, Ross C, Graham J, Luqmani R. Chronic primary vasculitis in children: a new research opportunity. CRAJ. 2012;22:10–11.
-
- Huber AM, Giannini EH, Bowyer SL, Kim S, Lang B, Lindsley CB, Pachman LM, Pilkington C, Reed AM, Rennebohm RM, et al. Protocols for the initial treatment of moderately severe juvenile dermatomyositis: results of a Children's arthritis and rheumatology research alliance consensus conference. Arthritis Care Res. 2010;62:219–225. doi: 10.1002/acr.20171. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
