

Neoadjuvant cisplatin and fluorouracil versus epirubicin, cisplatin, and capecitabine followed by resection in patients with oesophageal adenocarcinoma (UK MRC OE05): an open-label, randomised phase 3 trial
- PMID: 28784312
- PMCID: PMC5585417
- DOI: 10.1016/S1470-2045(17)30447-3
Neoadjuvant cisplatin and fluorouracil versus epirubicin, cisplatin, and capecitabine followed by resection in patients with oesophageal adenocarcinoma (UK MRC OE05): an open-label, randomised phase 3 trial
Abstract
Background: Neoadjuvant chemotherapy before surgery improves survival compared with surgery alone for patients with oesophageal cancer. The OE05 trial assessed whether increasing the duration and intensity of neoadjuvant chemotherapy further improved survival compared with the current standard regimen.
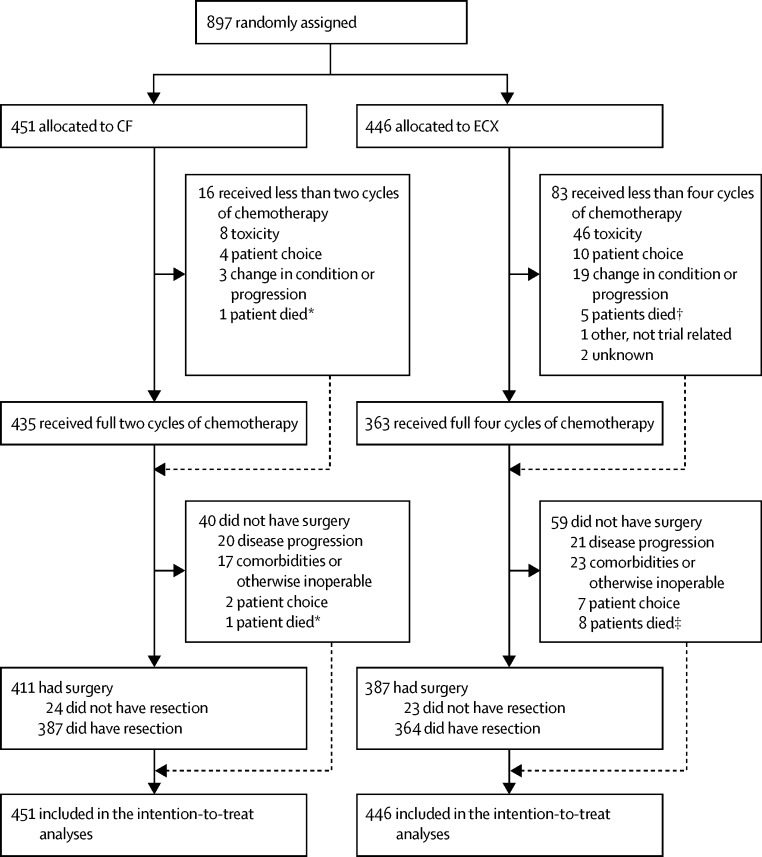
Methods: OE05 was an open-label, phase 3, randomised clinical trial. Patients with surgically resectable oesophageal adenocarcinoma classified as stage cT1N1, cT2N1, cT3N0/N1, or cT4N0/N1 were recruited from 72 UK hospitals. Eligibility criteria included WHO performance status 0 or 1, adequate respiratory, cardiac, and liver function, white blood cell count at least 3 × 109 cells per L, platelet count at least 100 × 109 platelets per L, and a glomerular filtration rate at least 60 mL/min. Participants were randomly allocated (1:1) using a computerised minimisation program with a random element and stratified by centre and tumour stage, to receive two cycles of cisplatin and fluorouracil (CF; two 3-weekly cycles of cisplatin [80 mg/m2 intravenously on day 1] and fluorouracil [1 g/m2 per day intravenously on days 1-4]) or four cycles of epirubicin, cisplatin, and capecitabine (ECX; four 3-weekly cycles of epirubicin [50 mg/m2] and cisplatin [60 mg/m2] intravenously on day 1, and capecitabine [1250 mg/m2] daily throughout the four cycles) before surgery, stratified according to centre and clinical disease stage. Neither patients nor study staff were masked to treatment allocation. Two-phase oesophagectomy with two-field (abdomen and thorax) lymphadenectomy was done within 4-6 weeks of completion of chemotherapy. The primary outcome measure was overall survival, and primary and safety analyses were done in the intention-to-treat population. This trial is registered with the ISRCTN registry (number 01852072) and ClinicalTrials.gov (NCT00041262), and is completed.
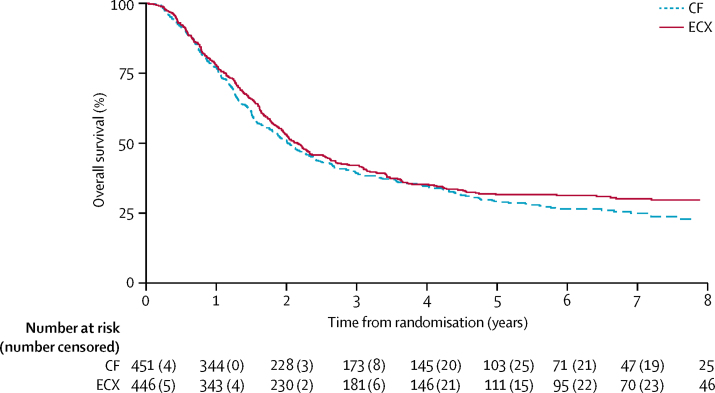
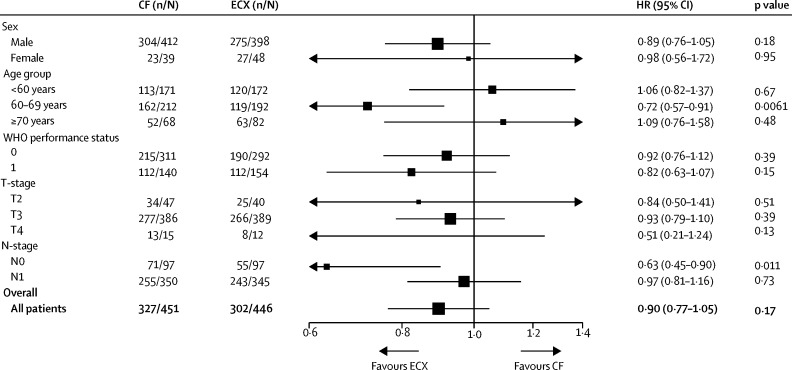
Findings: Between Jan 13, 2005, and Oct 31, 2011, 897 patients were recruited and 451 were assigned to the CF group and 446 to the ECX group. By Nov 14, 2016, 327 (73%) of 451 patients in the CF group and 302 (68%) of 446 in the ECX group had died. Median survival was 23·4 months (95% CI 20·6-26·3) with CF and 26·1 months (22·5-29·7) with ECX (hazard ratio 0·90 (95% CI 0·77-1·05, p=0·19). No unexpected chemotherapy toxicity was seen, and neutropenia was the most commonly reported event (grade 3 or 4 neutropenia: 74 [17%] of 446 patients in the CF group vs 101 [23%] of 441 people in the ECX group). The proportions of patients with postoperative complications (224 [56%] of 398 people for whom data were available in the CF group and 233 [62%] of 374 in the ECX group; p=0·089) were similar between the two groups. One patient in the ECX group died of suspected treatment-related neutropenic sepsis.
Interpretation: Four cycles of neoadjuvant ECX compared with two cycles of CF did not increase survival, and cannot be considered standard of care. Our study involved a large number of centres and detailed protocol with comprehensive prospective assessment of health-related quality of life in a patient population confined to people with adenocarcinomas of the oesophagus and gastro-oesophageal junction (Siewert types 1 and 2). Alternative chemotherapy regimens and neoadjuvant chemoradiation are being investigated to improve outcomes for patients with oesophageal carcinoma.
Funding: Cancer Research UK and Medical Research Council Clinical Trials Unit at University College London.
Copyright © 2017 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Neoadjuvant chemotherapy in oesophageal adenocarcinoma.Lancet Oncol. 2017 Nov;18(11):e639. doi: 10.1016/S1470-2045(17)30812-4. Epub 2017 Oct 31. Lancet Oncol. 2017. PMID: 29208393 No abstract available.
-
Neoadjuvant chemotherapy in oesophageal adenocarcinoma.Lancet Oncol. 2017 Nov;18(11):e640. doi: 10.1016/S1470-2045(17)30813-6. Epub 2017 Oct 31. Lancet Oncol. 2017. PMID: 29208394 No abstract available.
-
Neoadjuvant chemotherapy in oesophageal adenocarcinoma - Authors' reply.Lancet Oncol. 2017 Nov;18(11):e641. doi: 10.1016/S1470-2045(17)30776-3. Epub 2017 Oct 31. Lancet Oncol. 2017. PMID: 29208395 No abstract available.
References
-
- Sjoquist KM, Burmeister BH, Smithers BM, for the Australasian Gastro-Intestinal Trials Group Survival after neoadjuvant chemotherapy or chemoradiotherapy for resectable oesophageal carcinoma: an updated meta-analysis. Lancet Oncol. 2011;12:681–692. - PubMed
-
- Ronellenfitsch U, Schwarzbach M, Hofheinz R. Preoperative chemo(radio)therapy versus primary surgery for gastroesophageal adenocarcinoma: systematic review with meta-analysis combining individual patient and aggregate data. Eur J Cancer. 2013;49:3149–3158. - PubMed
-
- Nygaard K, Hagen S, Hansen HS. Pre-operative radiotherapy prolongs survival in operable esophageal carcinoma: a randomized, multicenter study of pre-operative radiotherapy and chemotherapy. The second Scandinavian trial in esophageal cancer. World J Surg. 1992;16:1104–1110. - PubMed
-
- Apinop C, Puttisak P, Preecha N. A prospective study of combined therapy in esophageal cancer. Hepatogastroenterology. 1994;41:391–393. - PubMed
-
- Le Prise E, Etienne PL, Meunier B. A randomized study of chemotherapy, radiation therapy, and surgery versus surgery for localized squamous cell carcinoma of the esophagus. Cancer. 1994;73:1779–1784. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
