

Temporal divergence of changes in pain and pain-free grip strength after manual acupuncture or electroacupuncture: an experimental study in people with lateral epicondylalgia
- PMID: 28785304
- PMCID: PMC5543448
- DOI: 10.1186/s13020-017-0143-z
Temporal divergence of changes in pain and pain-free grip strength after manual acupuncture or electroacupuncture: an experimental study in people with lateral epicondylalgia
Abstract
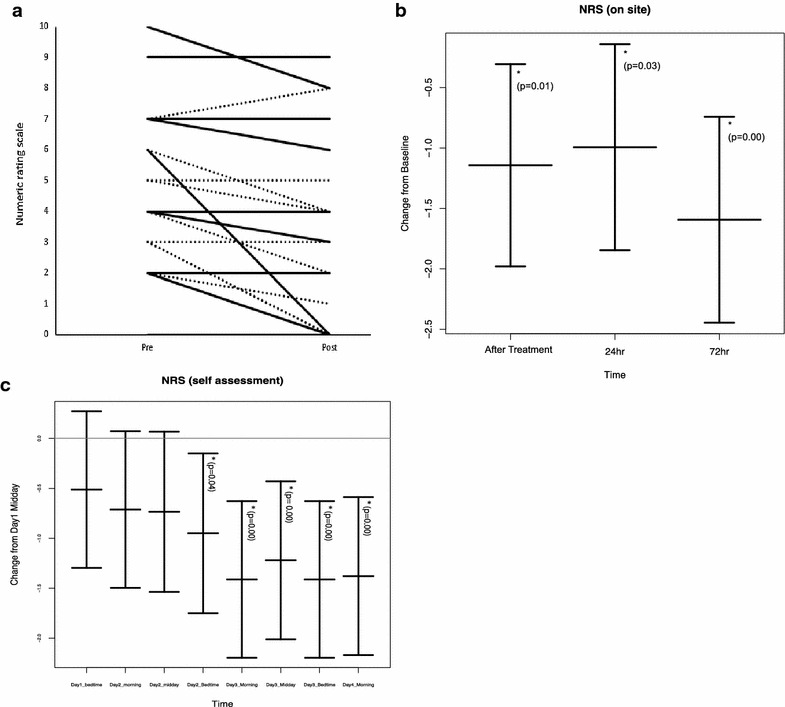
Background: The objective of this study was to examine, in individuals with lateral epicondylalgia (LE), the acute time course of acupuncture-induced hypoalgesia and change in pain-free grip strength (PFGS).
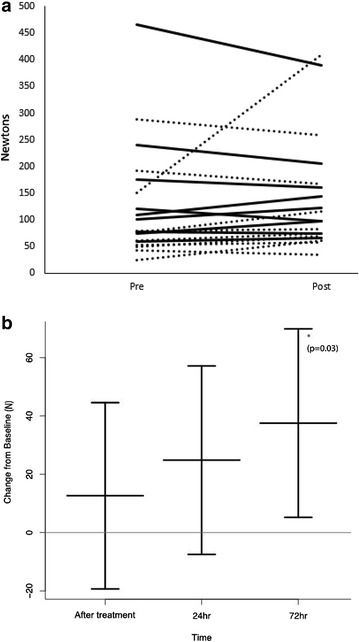
Methods: This was an experimental study, conducted at a single research center in Vancouver, BC. Twenty-one participants with unilateral LE lasting more than 6 weeks duration were enrolled. Participants received a single treatment of acupuncture (either electroacupuncture, 10-30 Hz, or manual acupuncture, assigned randomly). The primary outcome measure was pain level (0-10) during tendon loading (while making a fist) immediately after treatment, and over a 72 h follow-up period. Secondary outcome measures included pain-free grip strength (N).
Results: There was a small but statistically significant reduction in participants' perceived pain level immediately after acupuncture (mean improvement of 1.2, 95% CI 0.45-1.9). This change in pain was not accompanied by a change in PFGS. No difference was observed between the two types of acupuncture at any time point.
Conclusions: The use of acupuncture or electroacupuncture, as administered in the current study, is unlikely to acutely enhance the ability of people with LE to engage in pain-free rehabilitation exercise. Trial registration Registered February 25, 2015. ISRCTN14667535, http://www.isrctn.com/ISRCTN14667535.
Keywords: Acupuncture; Musculoskeletal; Tendinitis; Tendinopathy; Tendon.
Figures

Similar articles
-
Effects of manual acupuncture and electroacupuncture for lateral epicondylalgia of musculoskeletal origin: a systematic review and meta-analysis.Acupunct Med. 2021 Oct;39(5):405-422. doi: 10.1177/0964528420967364. Epub 2020 Dec 17. Acupunct Med. 2021. PMID: 33334116
-
Muscle energy technique versus corticosteroid injection for management of chronic lateral epicondylitis: randomized controlled trial with 1-year follow-up.Arch Phys Med Rehabil. 2013 Nov;94(11):2068-74. doi: 10.1016/j.apmr.2013.05.022. Epub 2013 Jun 22. Arch Phys Med Rehabil. 2013. PMID: 23796685 Clinical Trial.
-
Immediate effects of 2 types of braces on pain and grip strength in people with lateral epicondylalgia: a randomized controlled trial.J Orthop Sports Phys Ther. 2014 Feb;44(2):120-8. doi: 10.2519/jospt.2014.4744. Epub 2014 Jan 9. J Orthop Sports Phys Ther. 2014. PMID: 24405258 Clinical Trial.
-
Manipulation Therapy Relieved Pain More Rapidly Than Acupuncture among Lateral Epicondylalgia (Tennis Elbow) Patients: A Randomized Controlled Trial with 8-Week Follow-Up.Evid Based Complement Alternat Med. 2016;2016:3079247. doi: 10.1155/2016/3079247. Epub 2016 Apr 6. Evid Based Complement Alternat Med. 2016. PMID: 27143983 Free PMC article.
-
Analgesic effect of manual acupuncture and laser acupuncture for lateral epicondylalgia: a systematic review and meta-analysis.Am J Chin Med. 2014;42(6):1301-14. doi: 10.1142/S0192415X14500815. Am J Chin Med. 2014. PMID: 25384448
References
-
- du Toit C, Stieler M, Saunders R, et al. Diagnostic accuracy of power Doppler ultrasound in patients with chronic tennis elbow. Br J Sports Med. 2008;42:872–876. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
