

Tremelimumab-Induced Graves Hyperthyroidism
- PMID: 28785544
- PMCID: PMC5527187
- DOI: 10.1159/000464285
Tremelimumab-Induced Graves Hyperthyroidism
Abstract
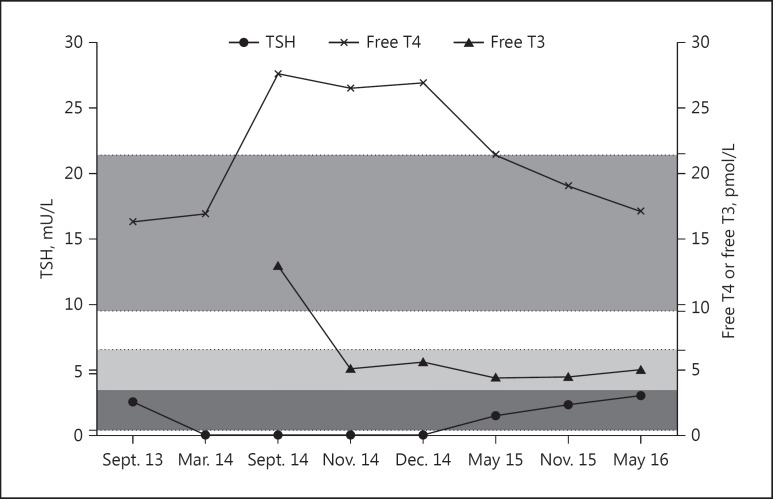
Tremelimumab and ipilimumab are monoclonal antibodies directed against the extracellular domain of cytotoxic T-lymphocyte-associated antigen 4 (CTLA-4) and have been used as immunotherapies against immune checkpoints that suppress T-cell activation. Anti-CTLA-4 antibody-based therapies have been shown to be effective in treating various cancers including metastatic melanoma. However, a few immune-related adverse events including hypophysitis and thyroid disorder have been reported, mostly developed within the first year of receiving treatment. We report a case of tremelimumab-induced Graves hyperthyroidism in a 55-year-old man who was diagnosed with metastatic melanoma after 8 years of tremelimumab therapy. He had no personal or family history of thyroid or autoimmune diseases. His biochemical profile was in keeping with Graves disease, with raised serum free thyroid hormones, suppressed thyroid-stimulating hormone concentration, and raised thyrotropin receptor antibody level. He was treated with carbimazole as part of the block and replace therapy, without complications. Tremelimumab therapy was temporarily discontinued and recommenced when he was rendered biochemically euthyroid. There has been no further relapse of Graves hyperthyroidism since the discontinuation of block and replace therapy. The mechanistic profile of anti-CTLA-4-induced thyroid dysfunction and the long-term endocrine safety of this therapeutic approach remain unclear. It is important to monitor thyroid functions in patients receiving anti-CTLA-4 therapies, as their effects on endocrine systems could be more latent or prolonged than the data from current clinical trials suggest. Antithyroid drug therapy was safe and effective alongside anti-CTLA-4 therapy without compromising antitumour treatment efficacy.
Keywords: Graves disease; Hyperthyroidism; Tremelimumab.
Figures
References
-
- Carreno BM, Collins M. The B7 family of ligands and its receptors: new pathways for costimulation and inhibition of immune responses. Annu Rev Immunol. 2002;20:29–53. - PubMed
-
- Drake CG, Jaffee E, Pardoll DM. Mechanisms of immune evasion by tumors. Adv Immunol. 2006;90:51. - PubMed
-
- Hodi FS, O'Day SJ, McDermott DF, Weber RW, Sosman JA, Haanen JB, Gonzalez R, Robert C, Schadendorf D, Hassel JC, Akerley W, van den Eertwegh AJ, Lutzky J, Lorigan P, Vaubel JM, Linette GP, Hogg D, Ottensmeier CH, Lebbé C, Peschel C, Quirt I, Clark JI, Wolchok JD, Weber JS, Tian J, Yellin MJ, Nichol GM, Hoos A, Urba WJ. Improved survival with ipilimumab in patients with metastatic melanoma. N Engl J Med. 2010;363:711–723. - PMC - PubMed
-
- Robert C, Thomas L, Bondarenko I, O'Day S, Weber J, Garbe C, Lebbe C, Baurain JF, Testori A, Grob JJ, Davidson N, Richrads J, Maio M, Hauschild A, Miller W, Gascon P, Lotem M, Harmankaya K, Ibrahim R, Francis S, Chen TT, Humphrey R, Hoos A, Wolchok J. Ipilimumab plus dacarbazine for previously untreated metastatic melanoma. N Engl J Med. 2011;364:2517–2526. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
