

Chronic total occlusions - Current techniques and future directions
- PMID: 28785642
- PMCID: PMC5497190
- DOI: 10.1016/j.ijcha.2015.02.002
Chronic total occlusions - Current techniques and future directions
Abstract
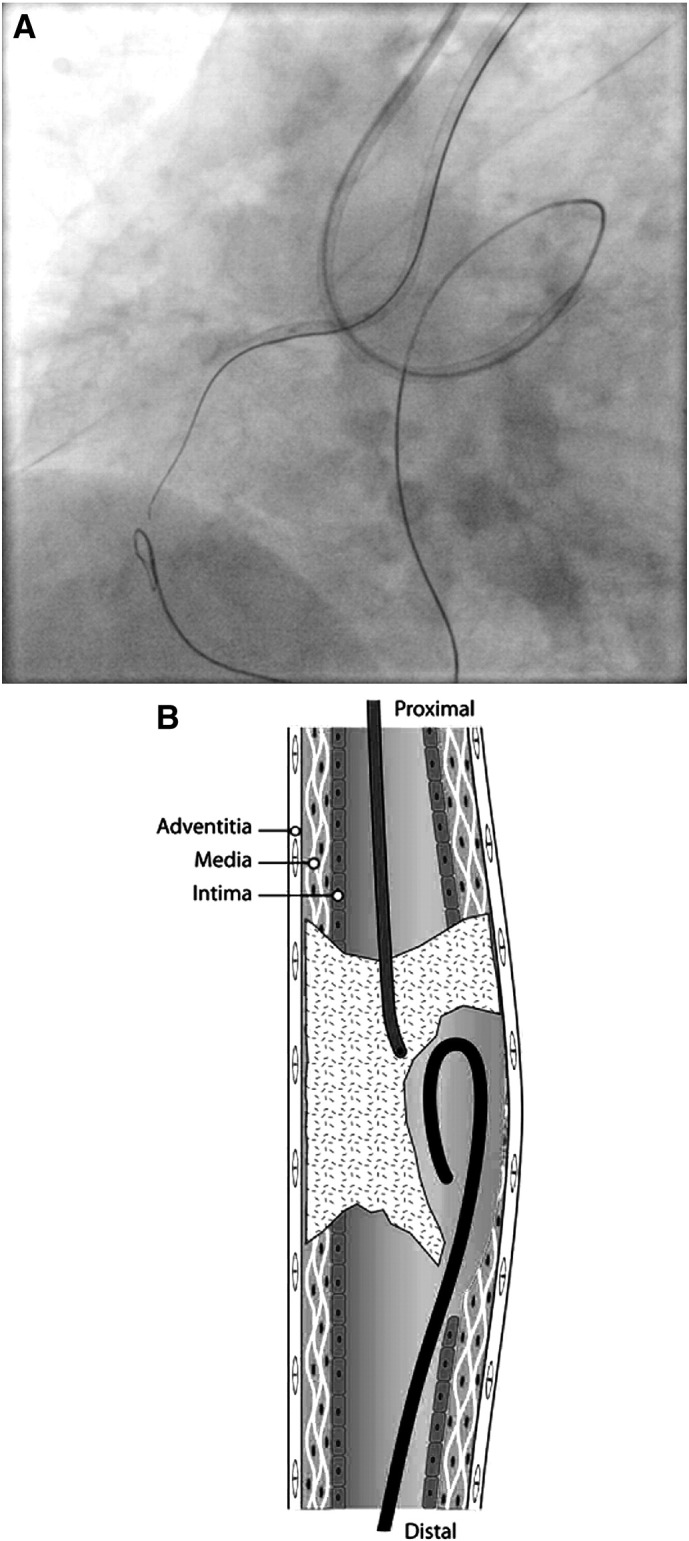
Chronic total occlusions (CTOs) of coronary arteries represent a common and significant challenge to interventional cardiology. Medical therapy is often regarded as an adequate long term strategy in the management of these lesions with surgical intervention for refractory symptoms. Extensive collateralisation is used as a marker of distal coronary perfusion, further reinforcing non-invasive strategies. This together with relatively low percutaneous success rates outside of specialised centres has meant that rates of percutaneous intervention have remained low. Increasing evidence suggests that CTOs are not a benign entity. Further, symptom control and quality of life improve significantly with successful percutaneous revascularisation. Both factors have reignited interest in percutaneous modalities. The Japanese have been pioneers in the field of CTO intervention although their success rates have been difficult to replicate. New techniques and equipment developed in North America offer an alternative to the Japanese approach. These techniques focus on time, radiation and contrast minimisation. This review will assess the histopathology of CTO and shifting paradigms in CTO treatment strategies.
Keywords: Antegrade; Chronic total occlusion; CrossBoss; Knuckle wire; Retrograde; Reverse CART; Stingray balloon; Techniques.
Figures
References
-
- Fefer P., Knudtson M.L., Cheema A.N., Galbraith P.D., Osherov A.B., Yalonetsky S. The Canadian Multicenter Chronic Total Occlusions Registry. Current perspectives on coronary chronic total occlusions. J Am Coll Cardiol. Mar 13 2012;59(11):991–997. - PubMed
-
- Christofferson R.D., Lehmann K.G., Martin G.V., Every N., Caldwell J.H., Kapadia S.R. Effect of chronic total coronary occlusion on treatment strategy. Am J Cardiol. May 1 2005;95(9):1088–1091. - PubMed
-
- Mohr F.W., Morice M.C., Kappetein A.P., Feldman T.E., Stahle E., Colombo A. Coronary artery bypass surgery versus percutaneous coronary intervention in patients with three vessel disease and left main coronary disease: 5 year follow up of the randomised, clinical SYNTAX trial. Lancet. Feb 23 2013;381(9867):629–638. - PubMed
-
- Claessen B.E., Dangas G.D., Weisz G., Witzenbichler B., Guagliumi G., Mockel M. Prognostic impact of a chronic total occlusion in a non-infarct-related artery in patients with ST-segment elevation myocardial infarction: 3-year results from the HORIZONS-AMI trial. Eur Heart J. Mar 2012;33(6):768–775. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
