

Percutaneous interventions in Fontan circulation
- PMID: 28785693
- PMCID: PMC5497275
- DOI: 10.1016/j.ijcha.2015.06.008
Percutaneous interventions in Fontan circulation
Abstract
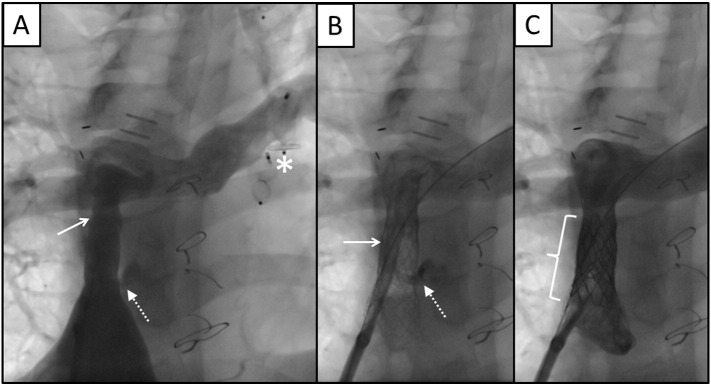
Introduction and objectives: Different percutaneous interventional procedures are needed to reach and maintain adequate anatomical and physiological conditions for the Fontan circulation. We aim to describe the experience gained at a children's hospital in such interventions, and to analyze the clinical outcomes.
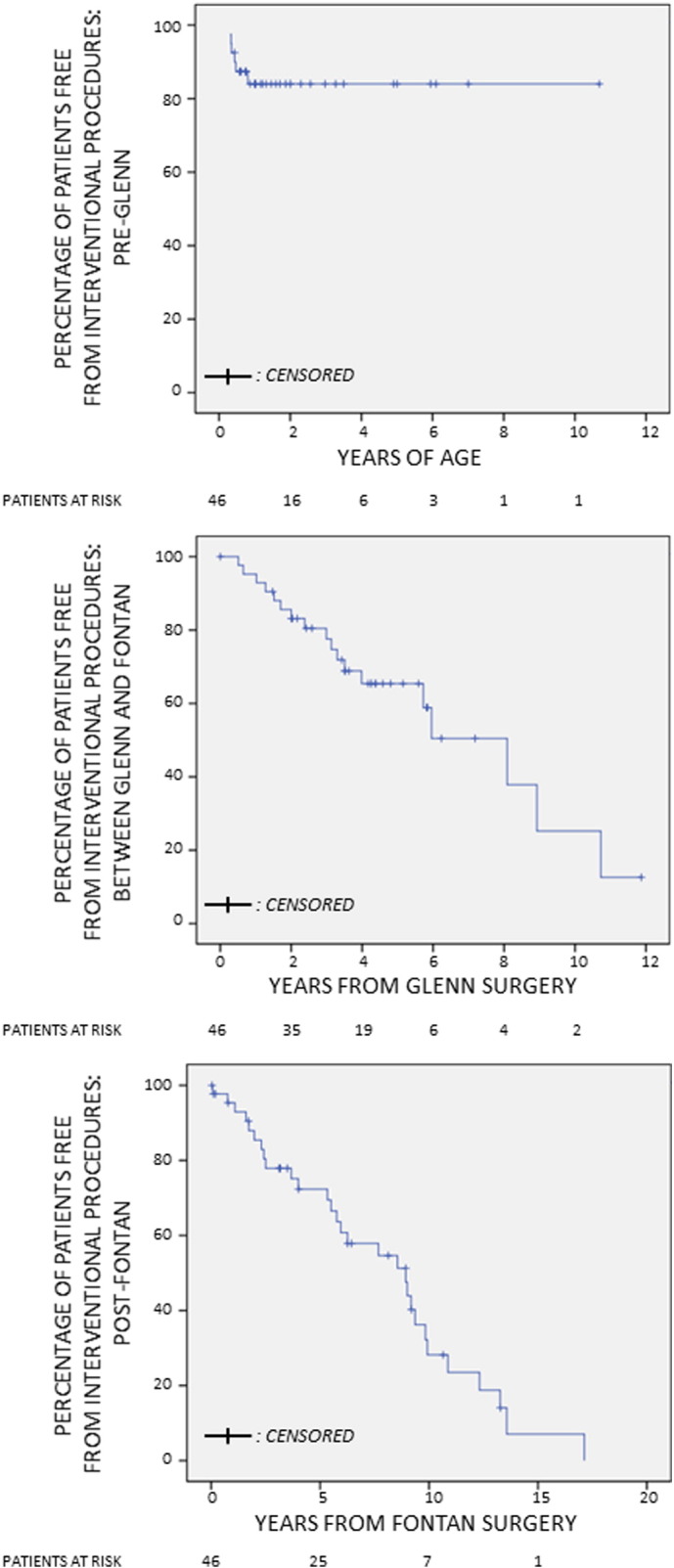
Methods: Retrospective study of all patients with Fontan circulation completed between 1995 and 2013. We analyzed the clinical characteristics and the different types of percutaneous interventions performed, considering three different periods of time: before Glenn surgery, between Glenn and Fontan surgeries, and after Fontan was completed. Survival and time to indication of percutaneous interventions in each period were analyzed, as well as the clinical situation at last follow-up.
Results: Of the 91 patients analyzed, 46 (50.5%) required percutaneous interventions. The most frequent procedures were pulmonary artery angioplasty and angioplasty of the Fontan conduit. Estimated survival at 10, 20 and 30 years of age was 96.2%, 94.7% and 89.4%, respectively. There were no significant differences in survival of patients undergoing percutaneous interventions or not. Overall survival and time to indication of percutaneous interventions were significantly lower in the group of patients with right morphology systemic ventricle. Patients with fenestrated Fontan required interventions more frequently. At the end of follow-up, 66 patients (72.5%) were asymptomatic, without significant differences between patients who underwent or did not undergo percutaneous interventions.
Conclusions: Interventional catheterization procedures are often necessary to reach and maintain the fragile Fontan circulation, mainly in patients with right morphology systemic ventricles and fenestrated Fontan conduits.
Keywords: CHD, congenital heart disease; Cardiac catheterization; Congenital heart disease; Fontan procedure; IVC, inferior vena cava; NYHA, New York Heart Association; PI, percutaneous intervention; Percutaneous intervention; SVC, superior vena cava; TCD, total cavopulmonary derivation.
Figures





References
-
- Mendoza A., Albert L., Ruiz E., Boni L., Ramos V., Velasco J.M. Operación de Fontan. Estudio de los factores hemodinámicos asociados a la evolución postoperatoria. Rev. Esp. Cardiol. 2012;65:356–362. - PubMed
-
- Cazzaniga M., Fernández L., Villagrá F. Pérez de León J, Gómez R, Sánchez P, et al. Operación modificada de Fontan o variantes efectuadas en un solo tiempo quirúrgico. Determinantes de la mortalidad. Rev. Esp. Cardiol. 2002;55:391–412. - PubMed
-
- Vyas H., Driscoll D.J., Cabalka A.K., Cetta F., Hagler D.J. Results of transcatheter Fontan fenestration to treat protein losing enteropathy. Catheter. Cardiovasc. Interv. 2007;69:584–589. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
