

What Should Define Preoperative Anemia in Primary THA?
- PMID: 28786087
- PMCID: PMC5638743
- DOI: 10.1007/s11999-017-5469-4
What Should Define Preoperative Anemia in Primary THA?
Abstract
Background: The use of tranexamic acid (TXA) in THA decreases the risk of transfusion after surgery. However, nearly 10% of patients still undergo a transfusion, which has been independently associated with an increased risk of complications. Preoperative anemia has been proven to be a strong predictor of transfusion after THA, but the ideal "cutoff" values in today's population that maximize sensitivity and specificity to predict transfusion have yet to be established.
Questions/purposes: (1) Which preoperative factors are associated with postoperative transfusion in the setting of TXA use? (2) If preoperative hemoglobin (Hgb) remains associated with transfusion, what are the best-supported preoperative Hgb cutoff values associated with increased transfusion after THA?
Methods: A retrospective chart analysis was performed from January 1, 2013, to January 1, 2015, on 558 primary THAs that met prespecified inclusion criteria. A multivariable logistic regression analysis model was used to identify independent factors associated with transfusion. Area under the receiver-operator curve (AUC) was used to determine the best-supported preoperative Hgb cut point across all participants, as well as adjusted by sex and TXA use. Overall, 60 patients with a blood transfusion were included and compared with 498 control subjects (11% risk of transfusion).
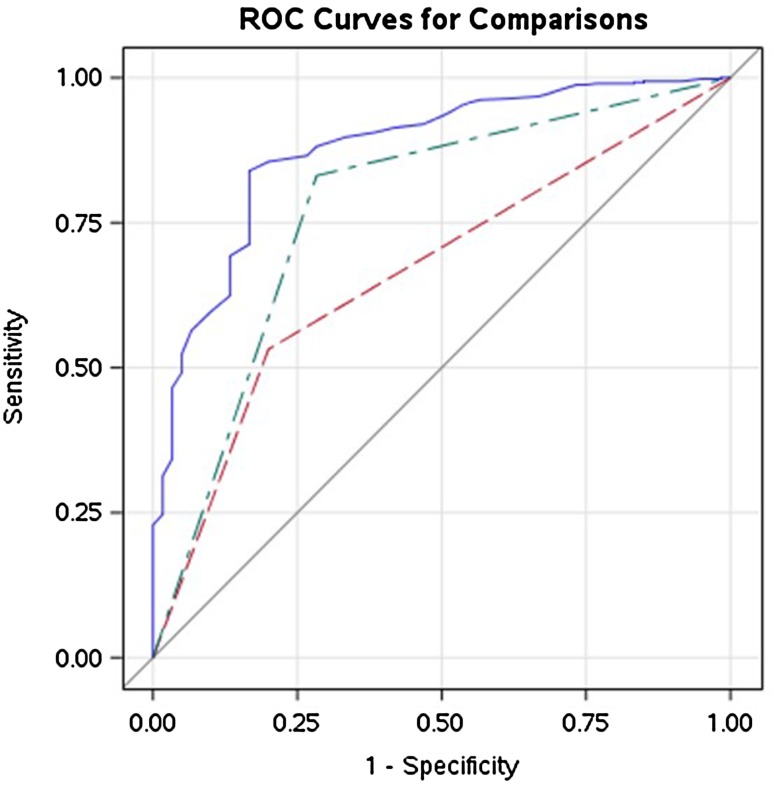
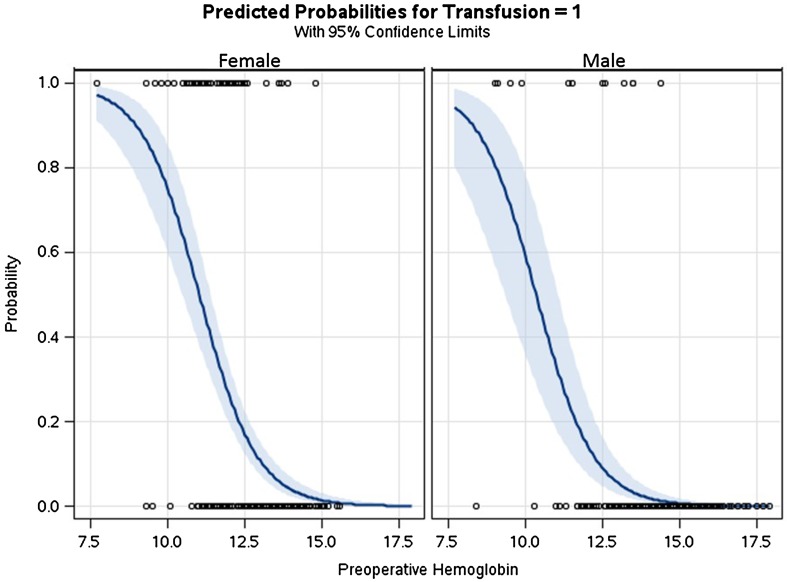
Results: After controlling for potential confounding variables such as age, sex, American Society of Anesthesiologist score, intravenous TXA (IV TXA) use, and preoperative Hgb, we found that patients with lower preoperative Hgb (g/dL per 1-unit decrease, odds ratio [OR], 2.6; 95% CI, 2.0-3.5; p < 0.001), female sex (vs male, OR, 4.2; 95% CI, 1.7-10.3; p = 0.002), and those unable to receive IV TXA (topical TXA/no TXA, OR, 13.5; 95% CI, 6.3-28.6; p < 0.001) were more likely to receive a transfusion. Of these, preoperative Hgb was found to be the variable most highly associated with transfusion (AUC, 0.876). A preoperative Hgb cutoff value of 12.6 g/dL maximized the AUC (0.876) for predicting transfusion across all patients unadjusted for baseline characteristics (sensitivity = 83, specificity = 84) with values of 12.5 g/dL (sensitivity = 85, specificity = 77) and 13.5 g/dL (sensitivity = 92, specificity = 77) for women and men, respectively.
Conclusions: The 1968 WHO definitions of anemia (preoperative Hgb < 13 g/dL for men and < 12 g/dL for women) used currently may underestimate patients at risk of transfusion after THA today. Further studies are needed to see if blood conservation referral decreases the risk of transfusion with preoperative treatment of anemia.
Level of evidence: Level III, therapeutic study.
Figures
Comment in
-
CORR Insights®: What Should Define Preoperative Anemia in Primary THA?Clin Orthop Relat Res. 2017 Nov;475(11):2692-2693. doi: 10.1007/s11999-017-5485-4. Epub 2017 Sep 2. Clin Orthop Relat Res. 2017. PMID: 28866845 Free PMC article. No abstract available.
Similar articles
-
Blood Transfusion in the Age of Tranexamic Acid: Who Needs a Type and Screen Before Total Hip Arthroplasty?J Arthroplasty. 2025 Jan;40(1):119-126. doi: 10.1016/j.arth.2024.06.053. Epub 2024 Jun 22. J Arthroplasty. 2025. PMID: 38914146
-
Low-volume formulation of intra-articular tranexamic acid, 25-ml tranexamic acid (2.5 g) plus 20-ml saline, is effective in decreasing blood transfusion rate in primary total knee replacement even without preoperative haemoglobin optimization.Blood Coagul Fibrinolysis. 2016 Sep;27(6):660-6. doi: 10.1097/MBC.0000000000000457. Blood Coagul Fibrinolysis. 2016. PMID: 27058218
-
Tranexamic Acid Benefits Total Joint Arthroplasty Patients Regardless of Preoperative Hemoglobin Value.J Arthroplasty. 2015 Dec;30(12):2098-101. doi: 10.1016/j.arth.2015.05.050. Epub 2015 Jun 3. J Arthroplasty. 2015. PMID: 26115982
-
The efficacy of topical tranexamic acid in total hip arthroplasty: a meta-analysis.BMC Musculoskelet Disord. 2016 Feb 16;17:81. doi: 10.1186/s12891-016-0923-0. BMC Musculoskelet Disord. 2016. PMID: 26878845 Free PMC article. Review.
-
Tranexamic Acid in Hip and Knee Arthroplasty.J Am Acad Orthop Surg. 2015 Dec;23(12):732-40. doi: 10.5435/JAAOS-D-14-00223. Epub 2015 Oct 22. J Am Acad Orthop Surg. 2015. PMID: 26493971 Review.
Cited by
-
Do Patients with Borderline Anemia Need Treatment before Total Hip Arthroplasty? A Propensity Score-Matched Cohort Study.Orthop Surg. 2024 Jan;16(1):123-131. doi: 10.1111/os.13955. Epub 2023 Dec 4. Orthop Surg. 2024. PMID: 38049380 Free PMC article.
-
Efficacy and cost-effectiveness of universal pre-operative iron studies in total hip and knee arthroplasty.J Orthop Surg Res. 2021 Aug 27;16(1):536. doi: 10.1186/s13018-021-02687-w. J Orthop Surg Res. 2021. PMID: 34452626 Free PMC article.
-
How are we defining preoperative anemia? A comparison of various anemia thresholds among patients undergoing short-construct lumbar spinal fusion.J Craniovertebr Junction Spine. 2025 Apr-Jun;16(2):188-194. doi: 10.4103/jcvjs.jcvjs_69_25. Epub 2025 Jul 3. J Craniovertebr Junction Spine. 2025. PMID: 40756486 Free PMC article.
-
Total hip arthroplasty was found to be safe in Jehovah's Witness patients: a multi-centered matched study.Arch Orthop Trauma Surg. 2024 Dec 31;145(1):103. doi: 10.1007/s00402-024-05740-5. Arch Orthop Trauma Surg. 2024. PMID: 39738842
-
Predisposing factors for allogeneic blood transfusion in patients with ankylosing spondylitis undergoing primary unilateral total hip arthroplasty: a retrospective study.J Orthop Surg Res. 2023 Jan 4;18(1):9. doi: 10.1186/s13018-022-03464-z. J Orthop Surg Res. 2023. PMID: 36597109 Free PMC article.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
