

Addressing the tuberculosis-depression syndemic to end the tuberculosis epidemic
- PMID: 28786792
- PMCID: PMC5759333
- DOI: 10.5588/ijtld.16.0584
Addressing the tuberculosis-depression syndemic to end the tuberculosis epidemic
Abstract
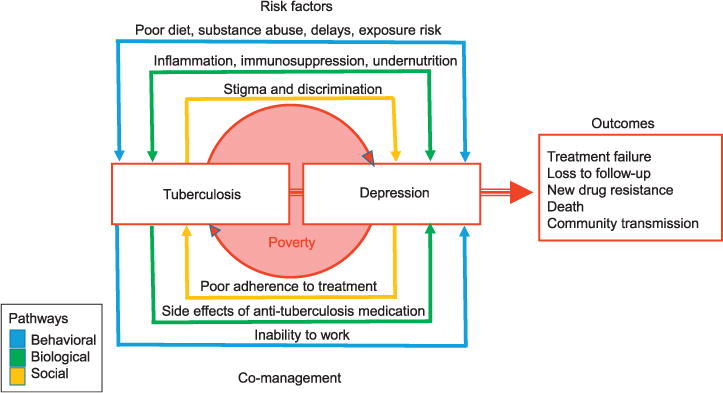
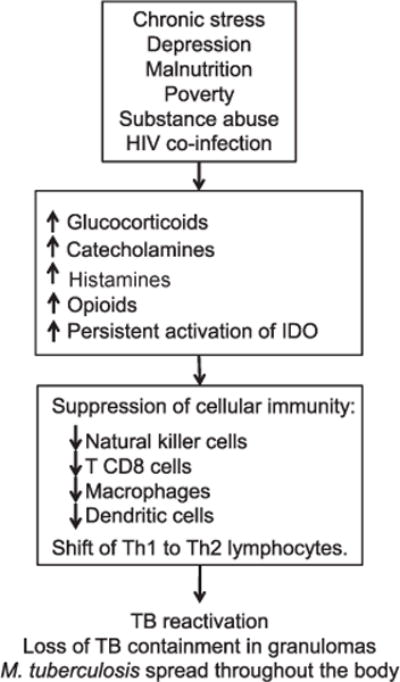
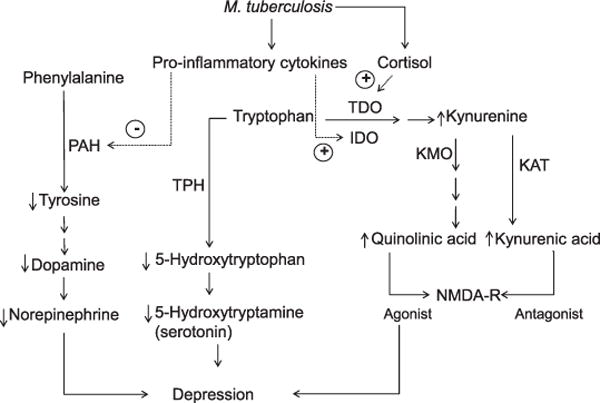
Tuberculosis (TB) and depression act synergistically via social, behavioral, and biological mechanisms to magnify the burden of disease. Clinical depression is a common, under-recognized, yet treatable condition that, if comorbid with TB, is associated with increased morbidity, mortality, community TB transmission, and drug resistance. Depression may increase risk of TB reactivation, contribute to disease progression, and/or inhibit the physiological response to anti-tuberculosis treatment because of poverty, undernutrition, immunosuppression, and/or negative coping behaviors, including substance abuse. Tuberculous infection and/or disease reactivation may precipitate depression as a result of the inflammatory response and/or dysregulation of the hypothalamic-pituitary-adrenal axis. Clinical depression may also be triggered by TB-related stigma, exacerbating other underlying social vulnerabilities, and/or may be attributed to the side effects of anti-tuberculosis treatment. Depression may negatively impact health behaviors such as diet, health care seeking, medication adherence, and/or treatment completion, posing a significant challenge for global TB elimination. As several of the core symptoms of TB and depression overlap, depression often goes unrecognized in individuals with active TB, or is dismissed as a normative reaction to situational stress. We used evidence to reframe TB and depression comorbidity as the 'TB-depression syndemic', and identified critical research gaps to further elucidate the underlying mechanisms. The World Health Organization's Global End TB Strategy calls for integrated patient-centered care and prevention linked to social protection and innovative research. It will require multidisciplinary approaches that consider conditions such as TB and depression together, rather than as separate problems and diseases, to end the global TB epidemic.
Conflict of interest statement
All other authors declare no conflicts of interest.
Figures
References
-
- World Health Organization. Global tuberculosis report. Geneva, Switzerland: WHO; 2016. (WHO/HTM/TB/2016.13). 2016.
-
- Duarte EC, Bierrenbach AL, Barbosa da Silva J, Jr, Tauil PL, de Fatima Duarte E. Factors associated with deaths among pulmonary tuberculosis patients: a case-control study with secondary data. J Epidemiol Community Health. 2009;63:233–238. - PubMed
-
- Johnson J, Kagal A, Bharadwaj R. Factors associated with drug resistance in pulmonary tuberculosis. Indian J Chest Dis Allied Sci. 2003;45:105–109. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
