

Higher incidence rates than previously known in tenosynovial giant cell tumors
- PMID: 28787222
- PMCID: PMC5694816
- DOI: 10.1080/17453674.2017.1361126
Higher incidence rates than previously known in tenosynovial giant cell tumors
Abstract
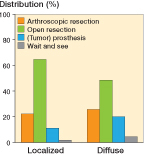
Background and purpose - Tenosynovial giant cell tumors (TGCT) are rare, benign tumors, arising in synovial lining of joints, tendon sheaths, or bursae. 2 types are distinguished: localized, either digits or extremity, and diffuse lesions. Current TGCT incidence is based on 1 single US-county study in 1980, with an incidence of 9 and 2 per million person-years in localized (including digits) and diffuse TGCT, respectively. We aim to determine nationwide and worldwide incidence rates (IR) in TGCT affecting digits, localized-extremity TGCT and diffuse-type TGCT. Material and methods - Over a 5-year period, the Dutch Pathology Registry (PALGA) identified 4,503 pathology reports on TGCT. Reports affecting digits were solely used for IR calculations. Reports affecting extremities were clinically evaluated. Dutch IRs were converted to world population IRs. Results - 2,815 (68%) digits, 933 (23%) localized-extremity and 390 (9%) diffuse-type TGCT were identified. Dutch IR in digits, localized-extremity, and diffuse-type TGCT was 34, 11 and 5 per million person-years, respectively. All 3 groups showed a female predilection and highest number of new cases in age category 40-59 years. The knee joint was most often affected: localized-extremity (46%) and diffuse-type (64%) TGCT, mostly treated with open resection: localized (65%) and diffuse (49%). Reoperation rate due to local recurrence for localized-extremity was 9%, and diffuse TGCT 23%. Interpretation - This first nationwide study and detailed analyses of IRs in TGCT estimated a worldwide IR in digits, localized-extremity and diffuse TGCT of 29, 10, and 4 per million person-years, respectively. Recurrence rate in diffuse type is 2.6 times higher, compared with localized extremity. TGCT is still considered a rare disease; however, it is more common than previously understood.
Figures






References
-
- Chiari C, Pirich C, Brannath W, Kotz R, Trieb K.. What affects the recurrence and clinical outcome of pigmented villonodular synovitis? Clin Orthop Rel Res 2006; 450: 172–8. - PubMed
-
- de St. Aubain Somerhausen N, Dal Cin P.. Gaint cell tumor of tendon sheath/diffuse-type giant cell tumor In: World Health Organization classification of tumors pathology and genetics of tumors of soft tissue and bone (Eds. Fletcher C D, Unni K K, Mertens F). Lyon: IARC Press; 2002. pp. 109–14.
-
- de St. Aubain Somerhausen N, van de Rijn M.. Tenosynovial giant cell tumor, localized type/diffuse type In: WHO classification of tumors of soft tissue and bone (Eds. Fletcher C D, Bridge J A, Hogendoorn P C, Mertens F). Lyon: IARC Press; 2013. pp. 100–3.
-
- Flandry F, Hughston J C, McCann S B, Kurtz D M.. Diagnostic features of diffuse pigmented villonodular synovitis of the knee. Clinical OrthopRel Res 1994. (298): 212–20. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases