

Evidence of advanced stage colorectal cancer with longer diagnostic intervals: a pooled analysis of seven primary care cohorts comprising 11 720 patients in five countries
- PMID: 28787432
- PMCID: PMC5589987
- DOI: 10.1038/bjc.2017.236
Evidence of advanced stage colorectal cancer with longer diagnostic intervals: a pooled analysis of seven primary care cohorts comprising 11 720 patients in five countries
Abstract
Background: The benefits from expedited diagnosis of symptomatic cancer are uncertain. We aimed to analyse the relationship between stage of colorectal cancer (CRC) and the primary and specialist care components of the diagnostic interval.
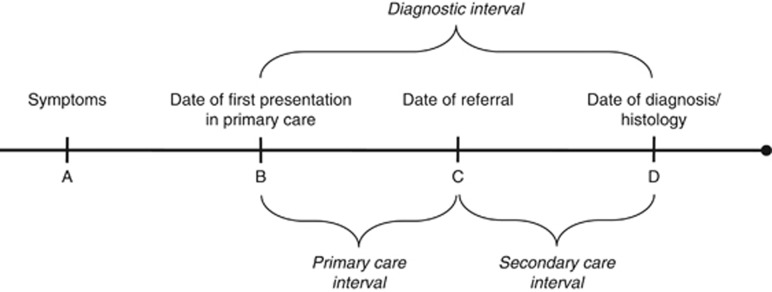
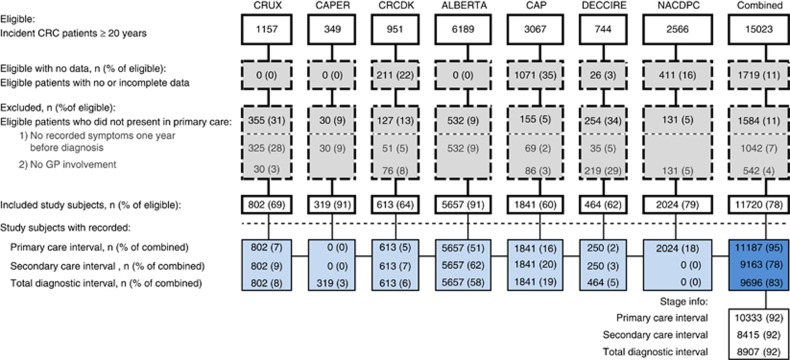
Methods: We identified seven independent data sets from population-based studies in Scotland, England, Canada, Denmark and Spain during 1997-2010 with a total of 11 720 newly diagnosed CRC patients, who had initially presented with symptoms to a primary care physician. Data were extracted from patient records, registries, audits and questionnaires, respectively. Data sets were required to hold information on dates in the diagnostic interval (defined as the time from the first presentation of symptoms in primary care until the date of diagnosis), symptoms at first presentation in primary care, route of referral, gender, age and histologically confirmed stage. We carried out reanalysis of all individual data sets and, using the same method, analysed a pooled individual patient data set.
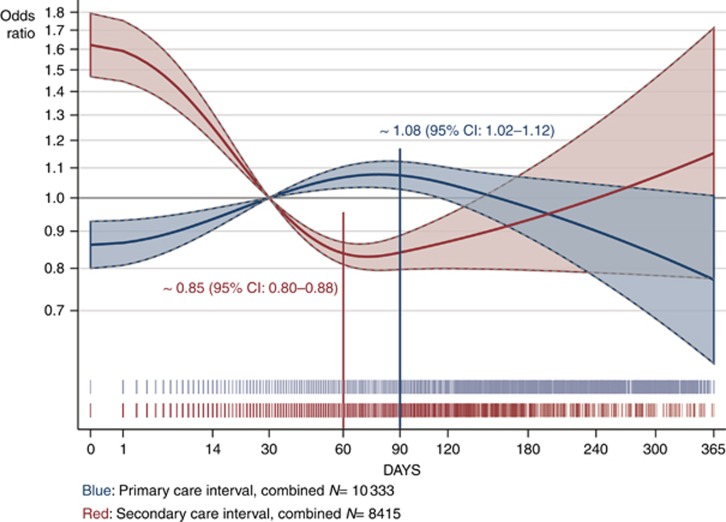
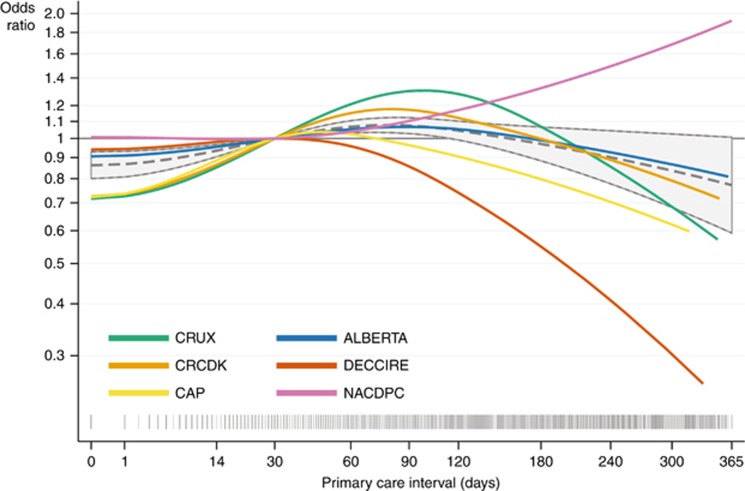
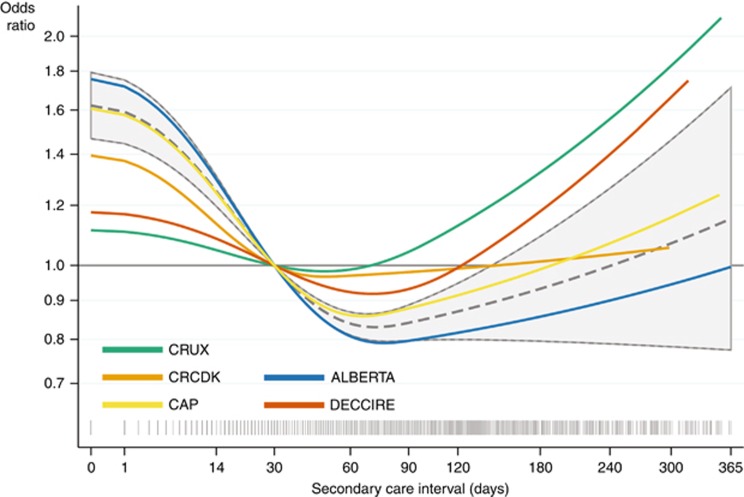
Results: The association between intervals and stage was similar in the individual and combined data set. There was a statistically significant convex (∩-shaped) association between primary care interval and diagnosis of advanced (i.e., distant or regional) rather than localised CRC (P=0.004), with odds beginning to increase from the first day on and peaking at 90 days. For specialist care, we saw an opposite and statistically significant concave (∪-shaped) association, with a trough at 60 days, between the interval and diagnosis of advanced CRC (P<0.001).
Conclusions: This study provides evidence that longer diagnostic intervals are associated with more advanced CRC. Furthermore, the study cannot define a specific 'safe' waiting time as the length of the primary care interval appears to have negative impact from day one.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Afzelius P, Zedeler K, Sommer H, Mouridsen HT, Blichert-Toft M (1994) Patient’s and doctor’s delay in primary breast cancer: prognostic implications. Acta Oncol 33: 345–351. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
