

High prevalence of CCDC103 p.His154Pro mutation causing primary ciliary dyskinesia disrupts protein oligomerisation and is associated with normal diagnostic investigations
- PMID: 28790179
- PMCID: PMC5771957
- DOI: 10.1136/thoraxjnl-2017-209999
High prevalence of CCDC103 p.His154Pro mutation causing primary ciliary dyskinesia disrupts protein oligomerisation and is associated with normal diagnostic investigations
Abstract
Rationale: Primary ciliary dyskinesia is a genetically heterogeneous inherited condition characterised by progressive lung disease arising from abnormal cilia function. Approximately half of patients have situs inversus. The estimated prevalence of primary ciliary dyskinesia in the UK South Asian population is 1:2265. Early, accurate diagnosis is key to implementing appropriate management but clinical diagnostic tests can be equivocal.
Objectives: To determine the importance of genetic screening for primary ciliary dyskinesia in a UK South Asian population with a typical clinical phenotype, where standard testing is inconclusive.
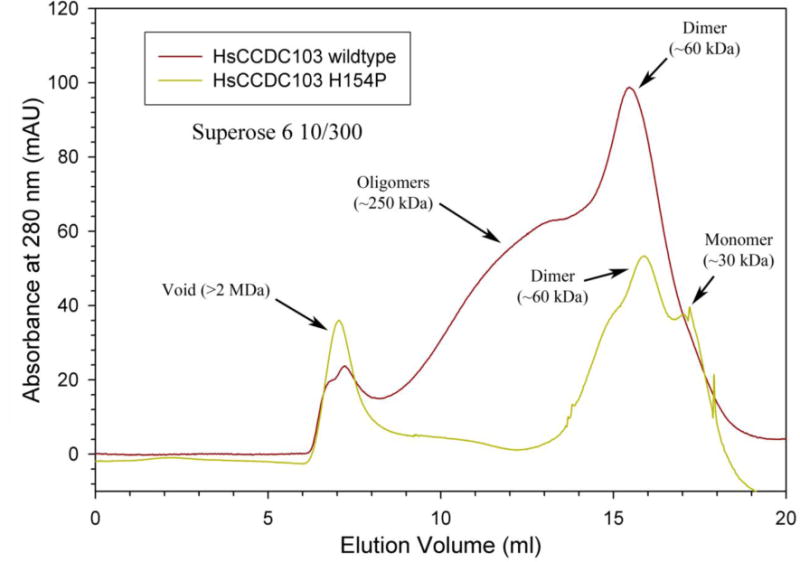
Methods: Next-generation sequencing was used to screen 86 South Asian patients who had a clinical history consistent with primary ciliary dyskinesia. The effect of a CCDC103 p.His154Pro missense variant compared with other dynein arm-associated gene mutations on diagnostic/phenotypic variability was tested. CCDC103 p.His154Pro variant pathogenicity was assessed by oligomerisation assay.
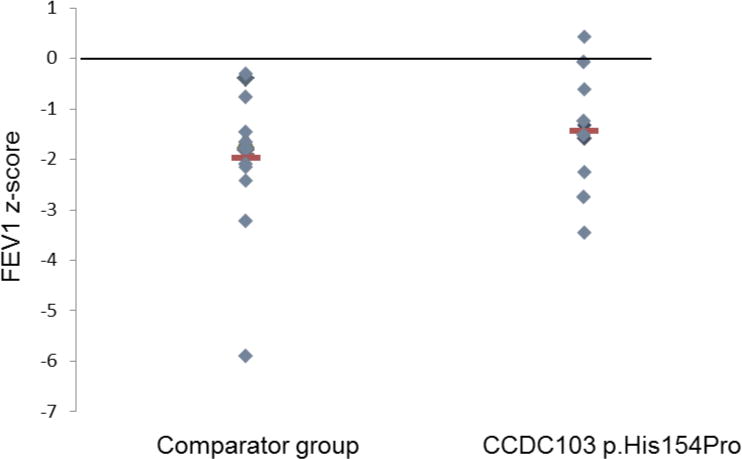
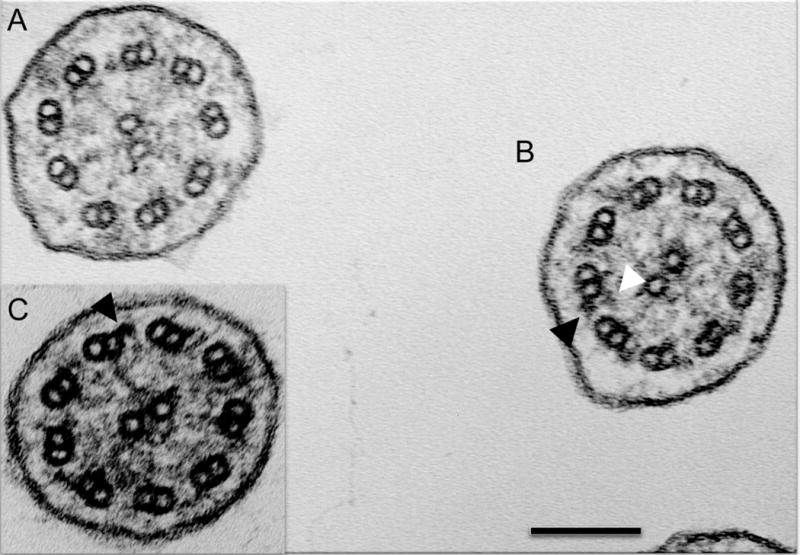
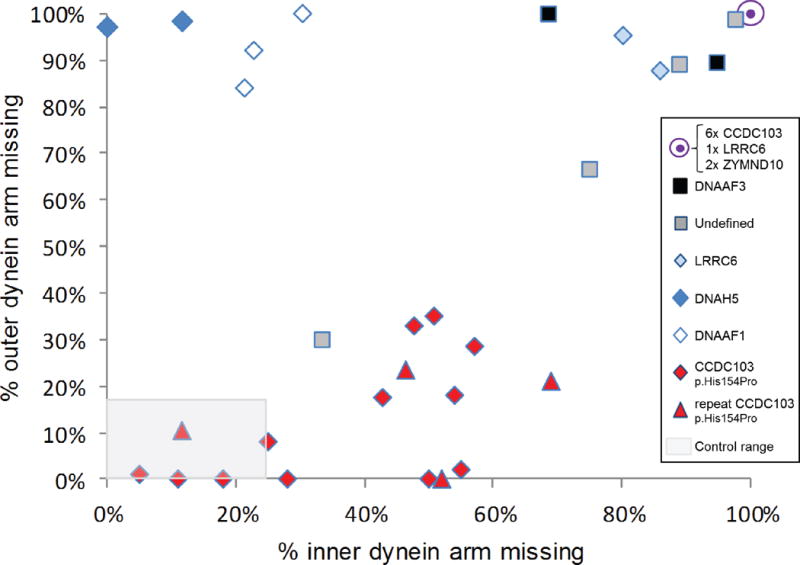
Results: Sixteen of 86 (19%) patients carried a homozygous CCDC103 p.His154Pro mutation which was found to disrupt protein oligomerisation. Variable diagnostic test results were obtained including normal nasal nitric oxide levels, normal ciliary beat pattern and frequency and a spectrum of partial and normal dynein arm retention. Fifteen (94%) patients or their sibling(s) had situs inversus suggesting CCDC103 p.His154Pro patients without situs inversus are missed.
Conclusions: The CCDC103 p.His154Pro mutation is more prevalent than previously thought in the South Asian community and causes primary ciliary dyskinesia that can be difficult to diagnose using pathology-based clinical tests. Genetic testing is critical when there is a strong clinical phenotype with inconclusive standard diagnostic tests.
Keywords: CCDC103; cilia; diagnosis; genetic testing.; mutation; primary ciliary dyskinesia; respiratory tract.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
Figures
Comment in
-
Primary ciliary dyskinesia: keep it on your radar.Thorax. 2018 Feb;73(2):101-102. doi: 10.1136/thoraxjnl-2017-210776. Epub 2017 Nov 13. Thorax. 2018. PMID: 29133352 Free PMC article. No abstract available.
References
-
- O’Callaghan C, Chetcuti P, Moya E. High prevalence of primary ciliary dyskinesia in a British Asian population. Arch Dis Child. 2010;95(1):51–2. - PubMed
-
- Shah A, Shoemark A, MacNeill SJ, et al. A longitudinal study characterising a large adult primary ciliary dyskinesia population. Eur Respir J. 2016;48(2):441–50. - PubMed
-
- Lucas JS, Barbato A, Collins SA, Goutaki M, Behan L, Caudri D, Dell S, Eber E, Escudier E, Hirst RA, Hogg C, Jorissen M, Latzin P, Legendre M, Leigh MW, Midulla F, Nielsen KG, Omran H, Papon JF, Pohunek P, Redfern B, Rigau D, Rindlisbacher BF, Shoemark A, Snijders D, Tonia T, Titieni A, Walker WT, Werner C, Bush A, Kuehni CE. ERS Task Force guideline for the diagnosis of primary ciliary dyskinesia. Eur Resp J. 2016 in press.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases