

Surgical Approaches for Total Hip Arthroplasty
- PMID: 28790465
- PMCID: PMC5525517
- DOI: 10.4103/ortho.IJOrtho_317_16
Surgical Approaches for Total Hip Arthroplasty
Abstract
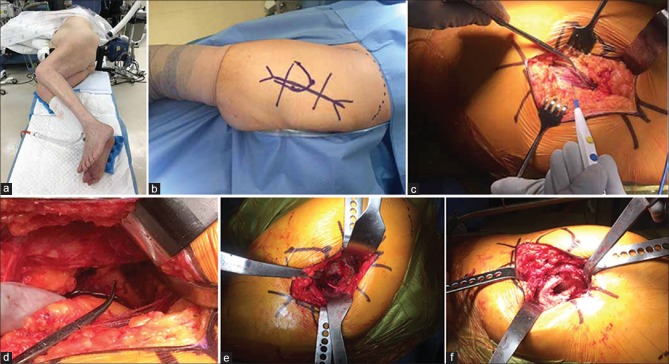
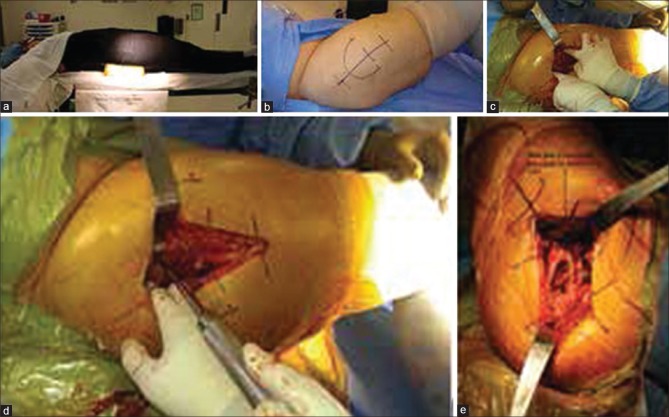
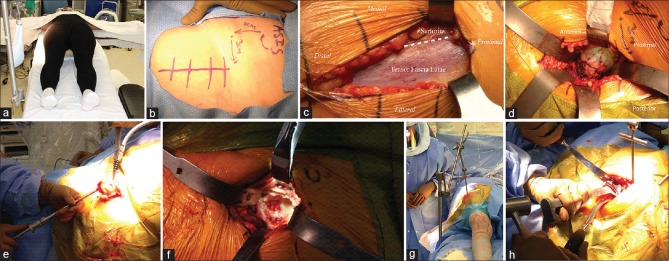
Total hip arthroplasty (THA) has become one of the most reliable and patient-requested surgical interventions in all medicine. The procedure can be performed using a variety of surgical approaches, but the posterior approach, direct lateral approach, and direct anterior approach are by far the most common across the globe. This article highlights the history and technique for each of these common approaches. A review of outcomes and complications for each approach are also provided. Each approach has its own unique advantages and disadvantages, but all can be safely and successful utilized for THA. Strong, convincing, high-quality studies comparing the different approaches are lacking at this time. Surgeons are therefore recommended to choose whichever approach they are most comfortable and experienced using. Though not described here, THA can also be done using the anterolateral approach (also known as the Watson Jones approach) as well as the two-incision approach. In addition, recently, some surgeons are utilizing the so-called direct superior approach for THA. While these approaches are far less commonly utilized, they are recognized as viable alternatives to traditional approaches.
Keywords: Direct anterior approach; Hardinge approach; Moore approach; Orthopaedics; Smith-Petersen approach; Southern approach; Surgery; Surgical technique; arthroplasty; direct lateral approach; hip; osteotomy; posterior approach; replacement; total hip arthroplasty; transgluteal approach.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Felson DT, Lawrence RC, Dieppe PA, Hirsch R, Helmick CG, Jordan JM, et al. Osteoarthritis: New insights. Part 1: The disease and its risk factors. Ann Intern Med. 2000;133:635–46. - PubMed
-
- Hootman JM, Helmick CG. Projections of US prevalence of arthritis and associated activity limitations. Arthritis Rheum. 2006;54:226–9. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical