

Current Concepts in Acetabular Positioning in Total Hip Arthroplasty
- PMID: 28790467
- PMCID: PMC5525519
- DOI: 10.4103/ortho.IJOrtho_144_17
Current Concepts in Acetabular Positioning in Total Hip Arthroplasty
Abstract
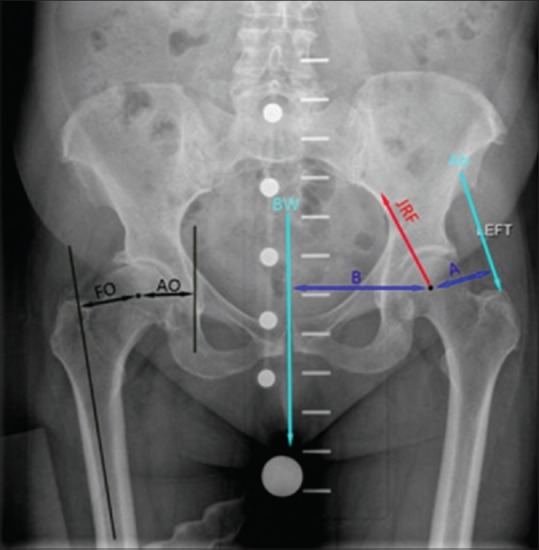
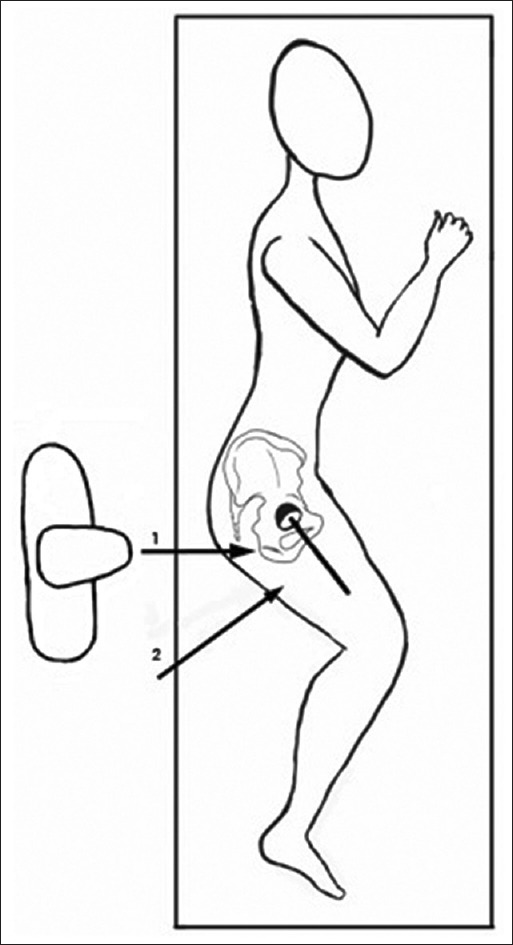
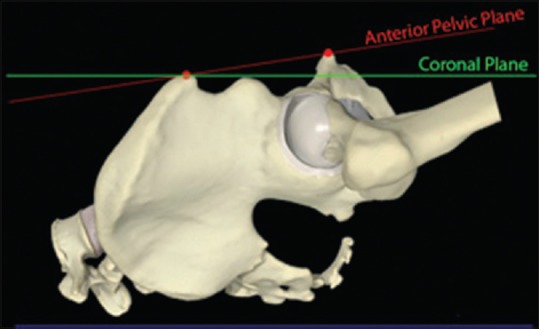
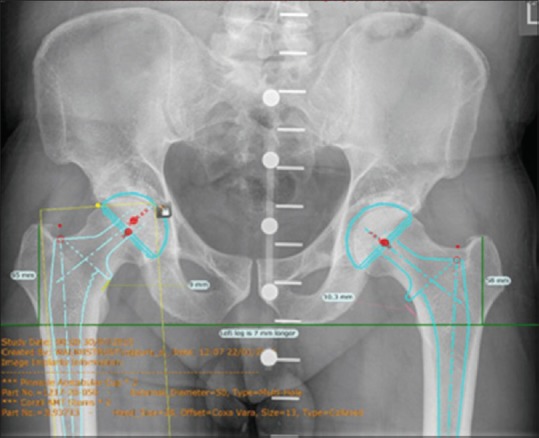
Being one of the most successful surgeries in the history of medicine, the indications for total hip arthroplasty have widened and are increasingly being offered to younger and fitter patients. This has also led to high expectations for longevity and outcomes. Acetabular cup position has a significant impact on the results of hip arthroplasty as it affects dislocation, abductor muscle strength, gait, limb lengths, impingement, noise generation, range of motion (ROM), wear, loosening, and cup failure. The variables in cup position are depth, height, and angular position (anteversion and inclination). The implications of change in depth of center of rotation (COR) are medialized versus anatomical positioning. As opposed to traditional medialization with beneficial effects on joint reaction force, the advantages of an anatomical position are increasingly recognized. The maintained acetabular offset offers advantages in terms of ROM, impingement, cortical rim press fit, and maintaining medial bone stock. The height of COR influences muscle activity and limb lengths and available bone stock for cup support. On the other hand, ideal angular position remains a matter of much debate and reliably achieving a target angular position remains elusive. This is not helped by variations in the way we describe angular position, with operative, radiologic, or anatomic definitions being used variably to describe anteversion and inclination. Furthermore, pelvic tilt plays a major role in functional positions of the acetabulum. In addition, commonly used techniques of positioning often do not inform us of the real orientation of the pelvis on operating table, with possibility of significant adduction, flexion, and external rotation of the pelvis being possibilities. This review article brings together the evidence on cup positioning and aims to provide a systematic and pragmatic approach in achieving the best position in individual cases.
Keywords: Acetabular cup position; Acetabulum; angular position; anteversion; arthroplasty; biomechanics; depth; height; hip; inclination; mediolateral; pelvic tilt; replacement; superoinferior.
Conflict of interest statement
There are no conflicts of interest.
Figures

References
-
- Jenkins PJ, Clement ND, Hamilton DF, Gaston P, Patton JT, Howie CR. Predicting the cost-effectiveness of total hip and knee replacement: A health economic analysis. Bone Joint J. 2013;95-B:115–21. - PubMed
-
- Lewinnek GE, Lewis JL, Tarr R, Compere CL, Zimmerman JR. Dislocations after total hip-replacement arthroplasties. J Bone Joint Surg Am. 1978;60:217–20. - PubMed
-
- Sakalkale DP, Sharkey PF, Eng K, Hozack WJ, Rothman RH. Effect of femoral component offset on polyethylene wear in total hip arthroplasty. Clin Orthop Relat Res. 2001;388:125–34. - PubMed
-
- Schmalzried TP, Shepherd EF, Dorey FJ, Jackson WO, dela Rosa M, Fa’vae F, et al. The John Charnley Award. Wear is a function of use, not time. Clin Orthop Relat Res. 2000;381:36–46. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials