

Risk factors for developing hypoxic respiratory failure in COPD
- PMID: 28790812
- PMCID: PMC5530070
- DOI: 10.2147/COPD.S140299
Risk factors for developing hypoxic respiratory failure in COPD
Abstract
Background: Hypoxemia is associated with worse outcomes in COPD. The aim of the study was to investigate the prevalence, incidence, and risk factors of hypoxic respiratory failure (HRF) in COPD.
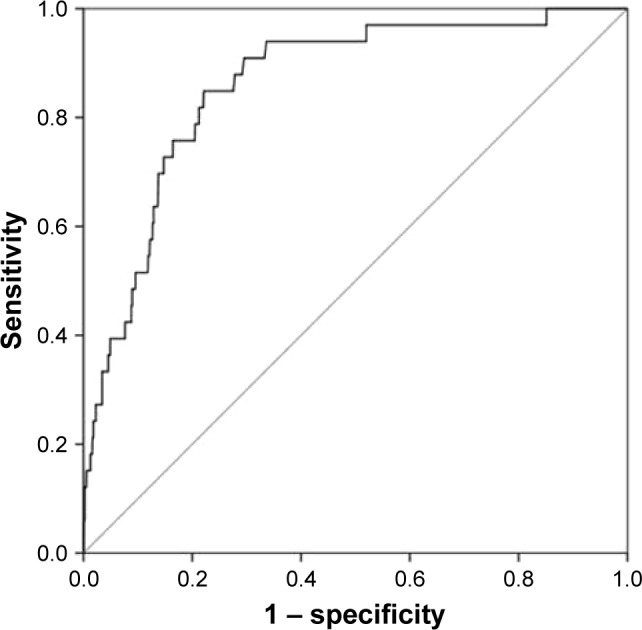
Patients and methods: This was a longitudinal analysis of data from the Swedish National Register of COPD. HRF was defined as resting saturation ≤88% or long-term oxygen therapy. Risk factors for developing HRF were analyzed using multiple logistic regression and receiver operating characteristic curve analysis.
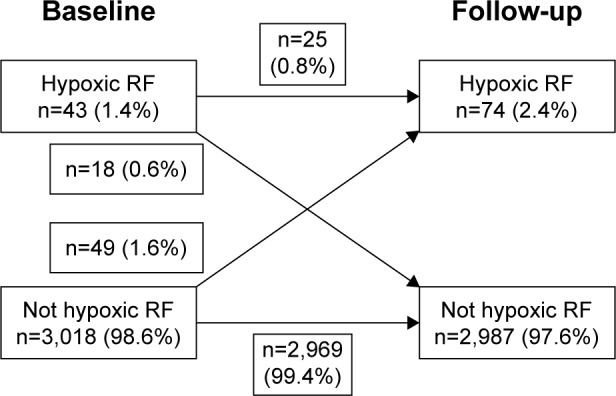
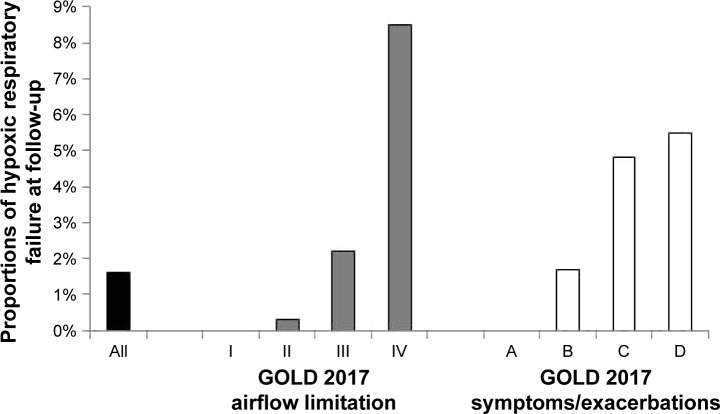
Results: A total of 3,061 patients were included; mean forced expiratory volume in 1 second was 1.47 L; mean age was 70 years; and 54% were females. Median follow-up time was 1.8 years (interquartile range 1.3-2.4 years). HRF was present in 43 (1.4%) patients at baseline and 74 (2.4%) patients at follow-up. Among patients without HRF at baseline, 49 (1.6%) developed HRF during follow-up. The risk was highest for patients in Global initiative for Chronic Obstructive Lung Disease (GOLD) 2017 stage IV or groups C or D at baseline. Developing HRF was independently predicted by lower forced expiratory volume in 1 second and lower COPD Assessment Test score, with a c-statistic of 0.84 (95% CI, 0.70-0.91). When the multivariable model used the GOLD 2017 variables stages I-IV and the dichotomized variables frequent exacerbations and COPD Assessment Test ≥10; the c-statistic increased slightly to 0.86 (95% CI, 0.80-0.92; P<0.0001).
Conclusion: In patients with COPD, the prevalence and incidence of HRF was low and was predicted well by more severe air flow limitation and worse health status. The risk is highest in patients with GOLD stage IV and GOLD groups C or D.
Keywords: COPD; GOLD 2017 assessment tool; health status; hypoxemia; hypoxic respiratory failure; longitudinal analysis; lung function; risk factors.
Conflict of interest statement
Disclosure The authors report no conflicts of interest in this work.
Figures
References
-
- Antonucci R, Berton E, Huertas A, Laveneziana P, Palange P. Exercise physiology in COPD. Monaldi Arch Chest Dis. 2003;59(2):134–139. - PubMed
-
- Chaouat A, Naeije R, Weitzenblum E. Pulmonary hypertension in COPD. Eur Respir J. 2008;32(5):1371–1385. - PubMed
-
- Vanier T, Dulfano J, Wu C, Desforges JF. Emphysema, hypoxia and the polycythemic response. N Engl J Med. 1963;269:169–178. - PubMed
-
- Garcia-Aymerich J, Monso E, Marrades RM, et al. Risk factors for hospitalization for a chronic obstructive pulmonary disease exacerbation. EFRAM study. Am J Respir Crit Care Med. 2001;164(6):1002–1007. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
