

Immunotargeting relapsed or refractory precursor B-cell acute lymphoblastic leukemia - role of blinatumomab
- PMID: 28790849
- PMCID: PMC5530848
- DOI: 10.2147/OTT.S103470
Immunotargeting relapsed or refractory precursor B-cell acute lymphoblastic leukemia - role of blinatumomab
Abstract
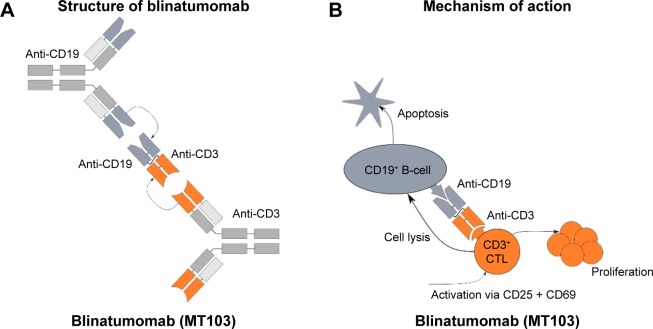
Patients with refractory or relapsed (R/R) acute lymphoblastic leukemia (ALL) have a dismal prognosis of around 5% long-term survival when treated with cytotoxic chemotherapy and allogenic stem cell transplantation. T-cell immunobased strategies open up new therapeutic perspectives. Blinatumomab is the first of a new class of antibody constructs that was labeled bispecific T-cell engager (BiTE): it consists of two single chain variable fragment connected with a flexible linker, one side binding CD3, the other CD19. The tight binding and the close proximity to the CD19-positive B-cells and leukemic cells leads to non-major histocompatibility complex-restricted T-cell activation, polyclonal T-cell expansion and direct target cell killing. Applied by continuous infusion, blinatumomab achieves morphological complete response rates ranging from 39% to 69% in R/R ALL patients (compared to 25% after second-line chemotherapy) with prolonged overall survival (blinatumomab median overall survival, 7.7 months vs chemotherapy, 4.0 months). In comparison to conventional cytotoxic second-line protocols blinatumomab has a favorable safety profile. The main adverse event is related to the mode of action of blinatumomab: the induction of a cytokine-release syndrome that can be managed by interruption and/or the application of steroids or tocilizumab. Another typical complication is the occurrence of neurological side effects, such as seizures and encephalopathy. This neurotoxicity is reversible after application of steroids and/or withdrawal of blinatumomab. Blinatumomab has proven to be a powerful therapeutic option in R/R ALL patients both adult and pediatric because of its efficacy and limited toxicity.
Keywords: R/R precursor B-cell ALL; T-cell; blinatumomab; immunotherapy.
Conflict of interest statement
Disclosure The authors report no conflicts of interest in this work.
Figures
References
-
- Bassan R, Hoelzer D. Modern therapy of acute lymphoblastic leukemia. J Clin Oncol. 2011;29(5):532–543. - PubMed
-
- Du XL, Chen Q. Recent advancements of bortezomib in acute lymphocytic leukemia treatment. Acta Haematol. 2013;129(4):207–214. - PubMed
-
- Klinger M, Benjamin J, Kischel R, Stienen S, Zugmaier G. Harnessing T cells to fight cancer with BiTE(R) antibody constructs – past developments and future directions. Immunol Rev. 2016;270(1):193–208. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
