

Rethinking Neuroprotection in Severe Traumatic Brain Injury: Toward Bedside Neuroprotection
- PMID: 28790967
- PMCID: PMC5523726
- DOI: 10.3389/fneur.2017.00354
Rethinking Neuroprotection in Severe Traumatic Brain Injury: Toward Bedside Neuroprotection
Abstract
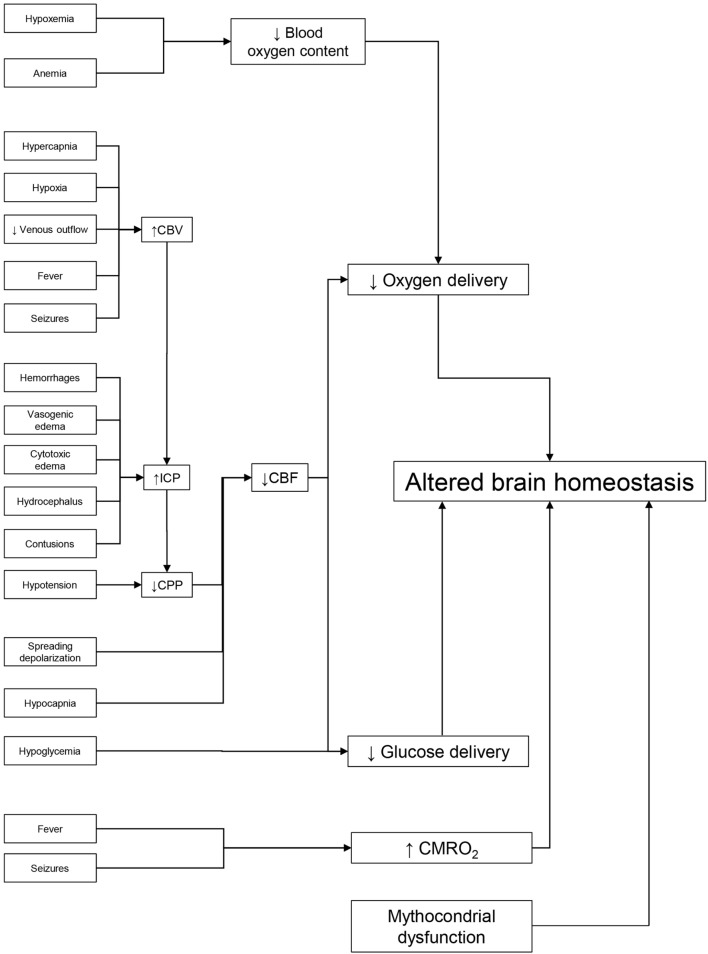
Neuroprotection after traumatic brain injury (TBI) is an important goal pursued strenuously in the last 30 years. The acute cerebral injury triggers a cascade of biochemical events that may worsen the integrity, function, and connectivity of the brain cells and decrease the chance of functional recovery. A number of molecules acting against this deleterious cascade have been tested in the experimental setting, often with preliminary encouraging results. Unfortunately, clinical trials using those candidate neuroprotectants molecules have consistently produced disappointing results, highlighting the necessity of improving the research standards. Despite repeated failures in pharmacological neuroprotection, TBI treatment in neurointensive care units has achieved outcome improvement. It is likely that intensive treatment has contributed to this progress offering a different kind of neuroprotection, based on a careful prevention and limitations of intracranial and systemic threats. The natural course of acute brain damage, in fact, is often complicated by additional adverse events, like the development of intracranial hypertension, brain hypoxia, or hypoperfusion. All these events may lead to additional brain damage and worsen outcome. An approach designed for early identification and prompt correction of insults may, therefore, limit brain damage and improve results.
Keywords: animal models; intensive care unit; multimodal monitoring; neuroprotection; traumatic brain injury.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources