

Influenza Vaccine Effectiveness in the United States during the 2015-2016 Season
- PMID: 28792867
- PMCID: PMC5727917
- DOI: 10.1056/NEJMoa1700153
Influenza Vaccine Effectiveness in the United States during the 2015-2016 Season
Abstract
Background: The A(H1N1)pdm09 virus strain used in the live attenuated influenza vaccine was changed for the 2015-2016 influenza season because of its lack of effectiveness in young children in 2013-2014. The Influenza Vaccine Effectiveness Network evaluated the effect of this change as part of its estimates of influenza vaccine effectiveness in 2015-2016.
Methods: We enrolled patients 6 months of age or older who presented with acute respiratory illness at ambulatory care clinics in geographically diverse U.S. sites. Using a test-negative design, we estimated vaccine effectiveness as (1-OR)×100, in which OR is the odds ratio for testing positive for influenza virus among vaccinated versus unvaccinated participants. Separate estimates were calculated for the inactivated vaccines and the live attenuated vaccine.
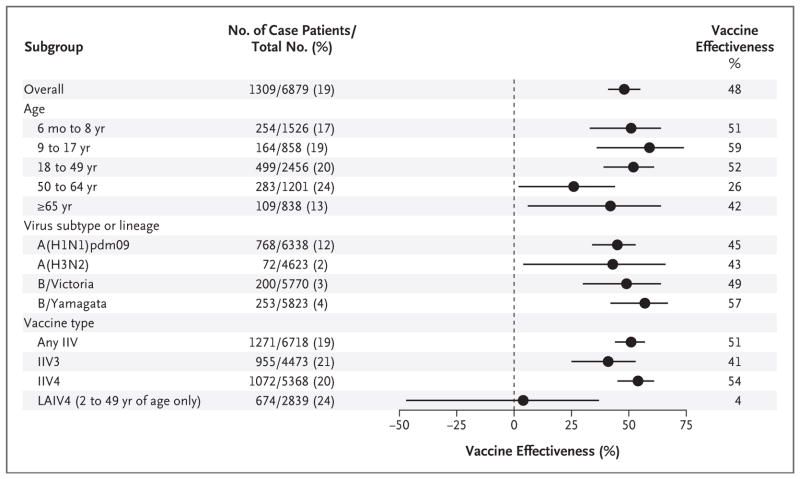
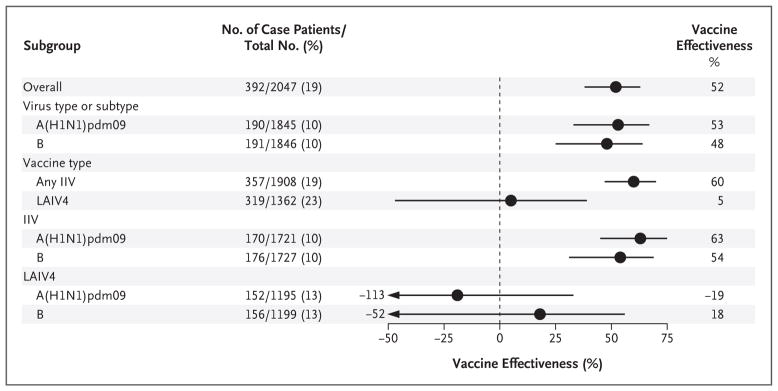
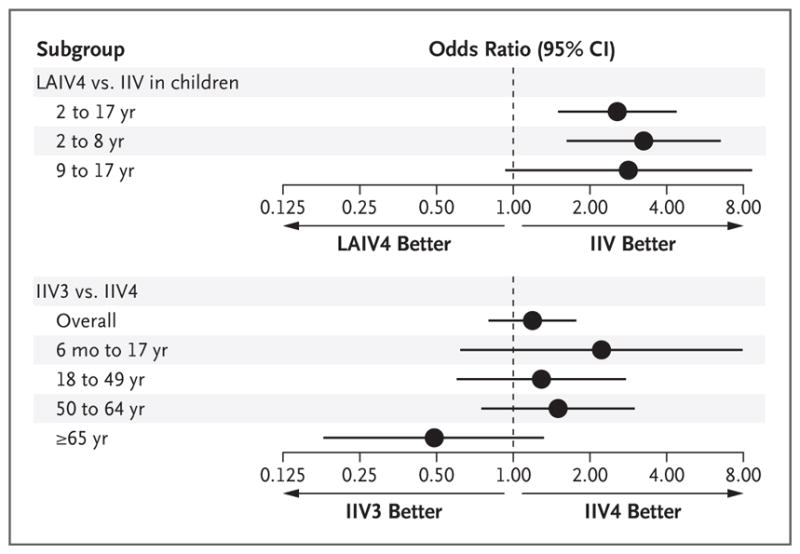
Results: Among 6879 eligible participants, 1309 (19%) tested positive for influenza virus, predominantly for A(H1N1)pdm09 (11%) and influenza B (7%). The effectiveness of the influenza vaccine against any influenza illness was 48% (95% confidence interval [CI], 41 to 55; P<0.001). Among children 2 to 17 years of age, the inactivated influenza vaccine was 60% effective (95% CI, 47 to 70; P<0.001), and the live attenuated vaccine was not observed to be effective (vaccine effectiveness, 5%; 95% CI, -47 to 39; P=0.80). Vaccine effectiveness against A(H1N1)pdm09 among children was 63% (95% CI, 45 to 75; P<0.001) for the inactivated vaccine, as compared with -19% (95% CI, -113 to 33; P=0.55) for the live attenuated vaccine.
Conclusions: Influenza vaccines reduced the risk of influenza illness in 2015-2016. However, the live attenuated vaccine was found to be ineffective among children in a year with substantial inactivated vaccine effectiveness. Because the 2016-2017 A(H1N1)pdm09 strain used in the live attenuated vaccine was unchanged from 2015-2016, the Advisory Committee on Immunization Practices made an interim recommendation not to use the live attenuated influenza vaccine for the 2016-2017 influenza season. (Funded by the Centers for Disease Control and Prevention and the National Institutes of Health.).
Figures
Comment in
-
Live, attenuated influenza vaccine demonstrated ineffective.J Pediatr. 2018 Jan;192:266-269. doi: 10.1016/j.jpeds.2017.10.055. J Pediatr. 2018. PMID: 29246354 No abstract available.
References
-
- DiazGranados CA, Dunning AJ, Kimmel M, et al. Efficacy of high-dose versus standard-dose influenza vaccine in older adults. N Engl J Med. 2014;371:635–45. - PubMed
-
- Belongia EA, Kieke BA, Donahue JG, et al. Effectiveness of inactivated influenza vaccines varied substantially with antigenic match from the 2004–2005 season to the 2006–2007 season. J Infect Dis. 2009;199:159–67. - PubMed
-
- Kelly H, Jacoby P, Dixon GA, et al. Vaccine effectiveness against laboratory-confirmed influenza in healthy young children: a case-control study. Pediatr Infect Dis J. 2011;30:107–11. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- UL1 TR000005/TR/NCATS NIH HHS/United States
- UL1 TR001857/TR/NCATS NIH HHS/United States
- U01 IP000466/IP/NCIRD CDC HHS/United States
- U01 IP000471/IP/NCIRD CDC HHS/United States
- U01 IP000474/IP/NCIRD CDC HHS/United States
- U01 IP000467/IP/NCIRD CDC HHS/United States
- U01 IP001034/IP/NCIRD CDC HHS/United States
- UL1 RR024153/RR/NCRR NIH HHS/United States
- U01 IP000473/IP/NCIRD CDC HHS/United States
- U01IP000473/ACL/ACL HHS/United States
- U01 IP001037/IP/NCIRD CDC HHS/United States
- U01 IP001038/IP/NCIRD CDC HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical