

On the path to 2025: understanding the Alzheimer's disease continuum
- PMID: 28793924
- PMCID: PMC5549378
- DOI: 10.1186/s13195-017-0283-5
On the path to 2025: understanding the Alzheimer's disease continuum
Abstract
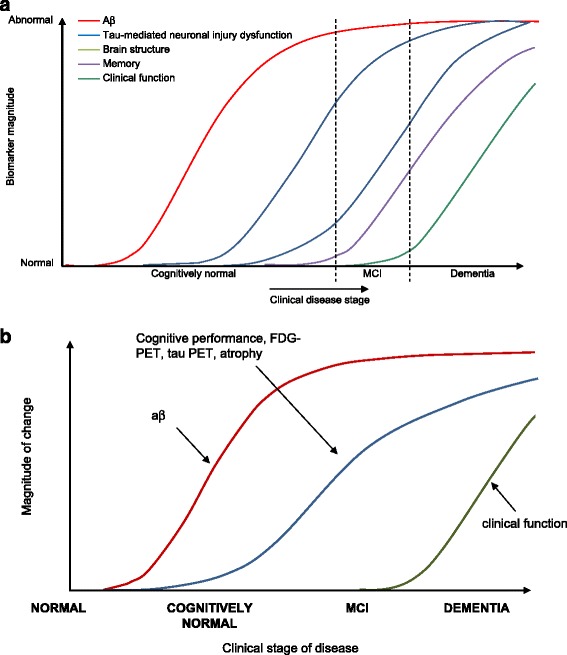
Basic research advances in recent years have furthered our understanding of the natural history of Alzheimer's disease (AD). It is now recognized that pathophysiological changes begin many years prior to clinical manifestations of disease and the spectrum of AD spans from clinically asymptomatic to severely impaired. Defining AD purely by its clinical presentation is thus artificial and efforts have been made to recognize the disease based on both clinical and biomarker findings. Advances with biomarkers have also prompted a shift in how the disease is considered as a clinico-pathophysiological entity, with an increasing appreciation that AD should not only be viewed with discrete and defined clinical stages, but as a multifaceted process moving along a seamless continuum. Acknowledging this concept is critical to understanding the development process for disease-modifying therapies, and for initiating effective diagnostic and disease management options. In this article, we discuss the concept of a disease continuum from pathophysiological, biomarker, and clinical perspectives, and highlight the importance of considering AD as a continuum rather than discrete stages. While the pathophysiology of AD has still not been elucidated completely, there is ample evidence to support researchers and clinicians embracing the view of a disease continuum in their study, diagnosis, and management of the disease.
Keywords: Alzheimer’s disease; Amyloid beta; Biomarker; Clinical; Cognitive impairment; Continuum; Dementia; Tau.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
PSA reports being a consultant to NeuroPhage, Merck, Roche, Novartis, Lundbeck, Biogen, Probiodrug, Anavex, and Abbvie; and receiving grants from Eli Lilly and Company, Janssen, the Alzheimer’s Association, and the NIH. JC reports providing consultation to Abbvie, Acadia, Actinogen, Alzheon, Anavex, Avanir, Axovant, Biogen-Idec, Boehringer-Ingelhiem, Bracket, Dart, Eisai, Eli Lilly and Company, Genentech, Lundbeck, MedAvante, Merck, Orion, Otsuka, Pfizer, Roche, Suven, and Takeda; and acknowledges the support of Keep Memory Alive and the National Institute of General Medical Sciences (Grant: P20GM109025). BD reports having received consultancy fees from Eli Lilly and Company and Boehringer-Ingelheim; and research funding for his Institution from Roche and Fondation Merck Avenir. LF reports receiving honoraria or consultation fees from Avid-Eli Lilly and Company, Astra-Zeneca, Axon Neuroscience, Baxter, Bayer, Boehringer-Ingelheim, Eisai, GE Health Care, Janssen-Cilag, Lundbeck, MerckSharpe & Dohme, Merz Pharma, Novartis, Pfizer, Schering-Plough, Schwabe Pharma, TAD Pharma, and Takeda; and receiving grants from Piramal and Novartis. CRJ reports having provided consulting services for Eli Lilly and Company; owning stock in Johnson and Johnson; and receiving research funding from the National Institutes of Health (R01-AG011378, RO1-AG041851, U01-AG06786, U01-AG024904, R01-AG37551, R01-AG043392, R01-NS092625) and the Alexander Family Alzheimer's Disease Research Professorship of the Mayo Foundation. RWJ reports honoraria and/or consultation fees from AC Immune, Eli Lilly and Company, Lundbeck, MSD, Novartis, Otsuka, and Roche; and his Institute has received grants for clinical trials from AC Immune, Acadia, Axovant, Biogen, Boehringer-Ingelheim, Eli Lilly and Company, Genentech, MSD, Pfizer, and Roche. JCM reports that neither he nor his family owns stock or has equity interest (outside of mutual funds or other externally directed accounts) in any pharmaceutical or biotechnology company; reports participating in the execution of trials of antidementia drugs from Eli Lilly and Company, Biogen, and Janssen; reports serving as a consultant for Eli Lilly and Company; reports receiving research support from Eli Lilly/Avid Radiopharmaceuticals; and reports receiving funding by NIH grants (P50AG005681; P01AG003991; P01AG026276, and UF01AG032438). RS reports receiving research funding from the National Institute on Aging, the Alzheimer’s Association, Fidelity Biosciences, and several philanthropic organizations, Eli Lilly and Co., and Janssen Pharmaceuticals; and has served as a paid consultant to Abbvie, Biogen, Bracket, Eisai, Genentech, Lundbeck, Merck, Otsuka, Roche, and Sanofi. SAD, BRM, and JR report being full-time employees and minor stockholders of Eli Lilly and Company. PS reports having acquired grant support from GE Healthcare, Danone Research, Piramal, and MERCK; having received in the past 2 years consultancy/speaker fees (paid to the institution) from Eli Lilly and Company, GE Healthcare, Novartis, Sanofi, Nutricia, Probiodrug, Biogen, Roche, Avraham, and EIP Pharma; and is editor-in-chief of Alzheimer’s Research & Therapy, but had no role in any part of the editorial process of this manuscript.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Glenner GG, Wong CW, Quaranta V, Eanes ED. The amyloid deposits in Alzheimer's disease: their nature and pathogenesis. Appl Pathol. 1984;2:357–69. - PubMed
-
- Brion JP, Passareiro H, Nunez J, Flament-Durand J. Mise en evidence de la immunologique de la protein tau au lesions de degeneresescence neurofibrillaire de la maladie. Arch Biol (Brux). 1985;95:229–35.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
