

Changes in Primary Noncardiac Diagnoses Over Time Among Elderly Cardiac Intensive Care Unit Patients in the United States
- PMID: 28794121
- PMCID: PMC5657300
- DOI: 10.1161/CIRCOUTCOMES.117.003616
Changes in Primary Noncardiac Diagnoses Over Time Among Elderly Cardiac Intensive Care Unit Patients in the United States
Abstract
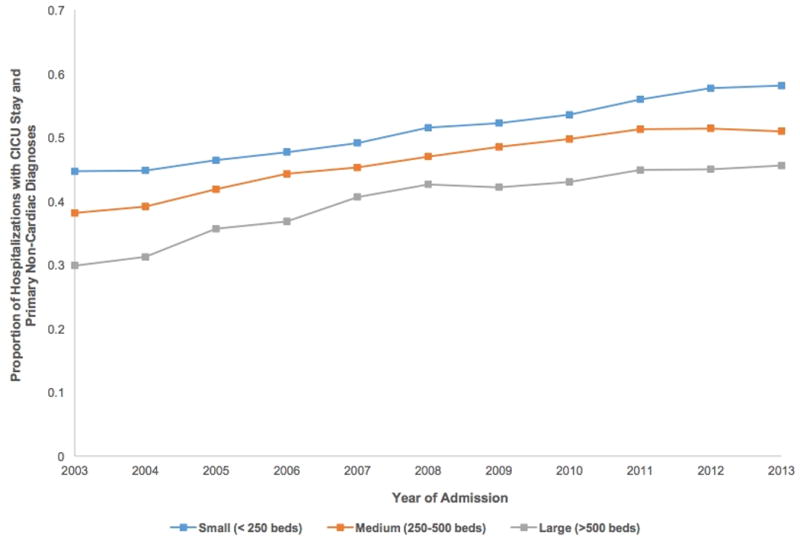
Background: Early reports suggest the number of cardiac intensive care unit (CICU) patients with primary noncardiac diagnoses is rising in the United States, but no national data currently exist. We examined changes in primary noncardiac diagnoses among elderly patients admitted to a CICU during the past decade.
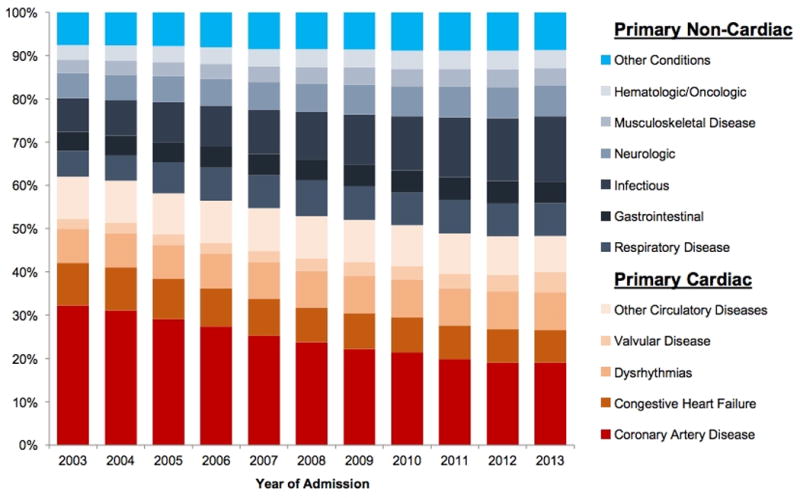
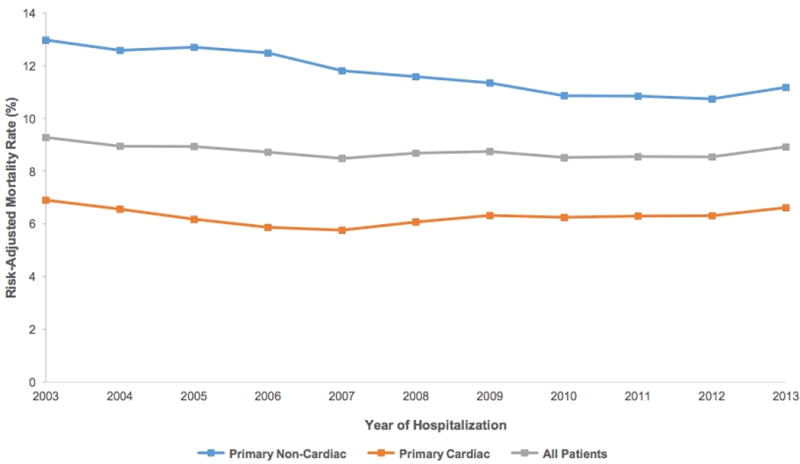
Methods and results: Using 2003 to 2013 Medicare data, we grouped elderly patients admitted to CICUs into 2 categories based on principal diagnosis at discharge: (1) primary noncardiac diagnoses and (2) primary cardiac diagnoses. We examined changes in patient demographics, comorbidities, procedure use, and risk-adjusted in-hospital mortality. Among 3.4 million admissions with a CICU stay, primary noncardiac diagnoses rose in prevalence from 38.0% to 51.7% between 2003 and 2013. The fastest rising primary noncardiac diagnoses were infectious diseases (7.8%-15.1%) and respiratory diseases (6.0%-7.6%; P<0.001 for both), whereas the fastest declining primary cardiac diagnosis was coronary artery disease (32.3%-19.0%; P<0.001). Simultaneously, the prevalence of both cardiovascular and noncardiovascular comorbidities rose: heart failure (13.9%-34.4%), pulmonary vascular disease (1.2%-7.1%), valvular heart disease (5.0%-9.8%), and renal failure (7.1%-19.6%; P<0.001 for all). As compared with those with primary cardiac diagnoses, elderly CICU patients with primary noncardiac diagnoses had higher rates of noncardiac procedure use and risk-adjusted in-hospital mortality (P<0.001 for all). Risk-adjusted in-hospital mortality declined slightly in the overall cohort from 9.3% to 8.9% (P<0.001).
Conclusions: More than half of all elderly patients with a CICU stay across the United States now have primary noncardiac diagnoses at discharge. These patients receive different types of care and have worse outcomes than patients with primary cardiac diagnoses. Our work has important implications for the development of appropriate training and staffing models for the future critical care workforce.
Keywords: coronary artery disease; critical care; health services research; heart failure; intensive care units.
© 2017 American Heart Association, Inc.
Conflict of interest statement
Figures
Comment in
-
Trends in Cardiac Critical Care: Reshaping the Cardiac Intensive Care Unit.Circ Cardiovasc Qual Outcomes. 2017 Aug;10(8):e004010. doi: 10.1161/CIRCOUTCOMES.117.004010. Circ Cardiovasc Qual Outcomes. 2017. PMID: 28794123 No abstract available.
References
-
- Zoll PM, Linenthal AJ, Gibson W, Paul MH, Norman LR. Termination of ventricular fibrillation in man by externally applied electric countershock. N Engl J Med. 1956;254:727–732. - PubMed
-
- Lown B, Amarasingham R, Neuman J. New method for terminating cardiac arrhythmias. Use of synchronized capacitor discharge. JAMA. 1962;182:548–555. - PubMed
-
- Julian DG. Treatment of cardiac arrest in acute myocardial ischaemia and infarction. Lancet. 1961;2:840–844. - PubMed
-
- Killip T, 3rd, Kimball JT. Treatment of myocardial infarction in a coronary care unit. A two year experience with 250 patients. Am J Cardiol. 1967;20:457–464. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
