

Quantitative Assessment of Coronary Microvascular Function: Dynamic Single-Photon Emission Computed Tomography, Positron Emission Tomography, Ultrasound, Computed Tomography, and Magnetic Resonance Imaging
- PMID: 28794138
- PMCID: PMC5678979
- DOI: 10.1161/CIRCIMAGING.117.006427
Quantitative Assessment of Coronary Microvascular Function: Dynamic Single-Photon Emission Computed Tomography, Positron Emission Tomography, Ultrasound, Computed Tomography, and Magnetic Resonance Imaging
Abstract
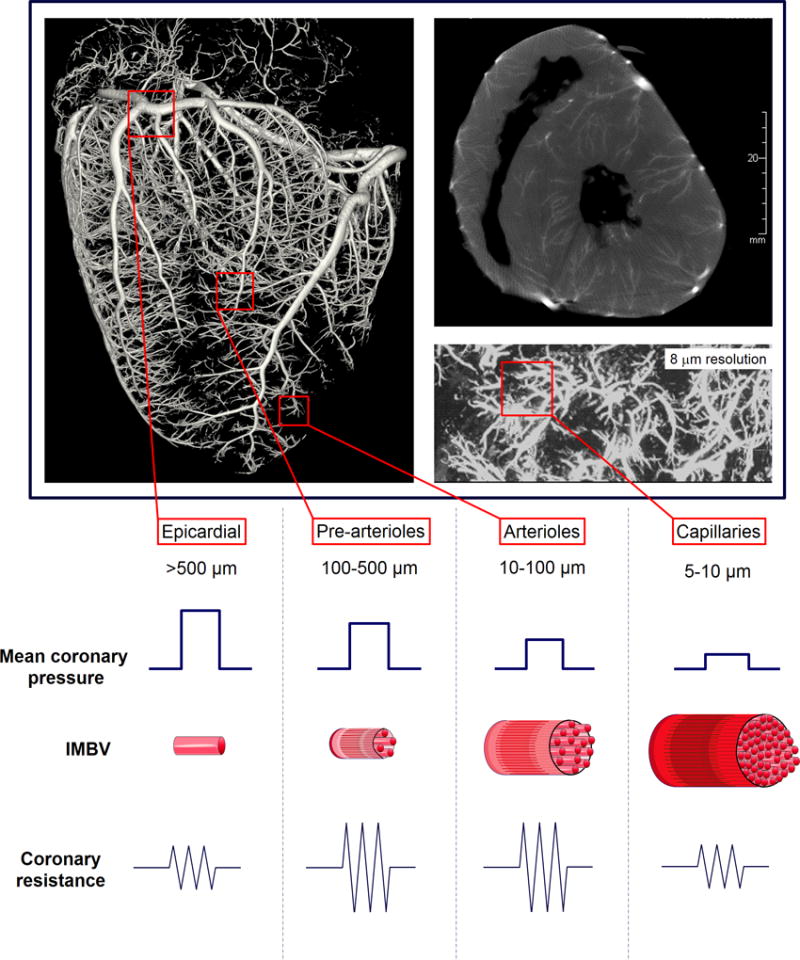
A healthy, functional microcirculation in combination with nonobstructed epicardial coronary arteries is the prerequisite of normal myocardial perfusion. Quantitative assessment in myocardial perfusion and determination of absolute myocardial blood flow can be achieved noninvasively using dynamic imaging with multiple imaging modalities. Extensive evidence supports the clinical value of noninvasively assessing indices of coronary flow for diagnosing coronary microvascular dysfunction; in certain diseases, the degree of coronary microvascular impairment carries important prognostic relevance. Although, currently positron emission tomography is the most commonly used tool for the quantification of myocardial blood flow, other modalities, including single-photon emission computed tomography, computed tomography, magnetic resonance imaging, and myocardial contrast echocardiography, have emerged as techniques with great promise for determination of coronary microvascular dysfunction. The following review will describe basic concepts of coronary and microvascular physiology, review available modalities for dynamic imaging for quantitative assessment of coronary perfusion and myocardial blood flow, and discuss their application in distinct forms of coronary microvascular dysfunction.
Keywords: coronary flow reserve; coronary microvascular function; microvascular dysfunction; myocardial blood flow; myocardial perfusion imaging.
© 2017 American Heart Association, Inc.
Figures
References
-
- Camici PG, Crea F. Coronary microvascular dysfunction. N Engl J Med. 2007;356:830–40. - PubMed
-
- Salerno M, Beller GA. Noninvasive assessment of myocardial perfusion. Circ Cardiovasc Imaging. 2009;2:412–24. - PubMed
-
- Mekkaoui C, Jadbabaie F, Dione DP, Meoli DF, Purushothaman K, Belardinelli L, Sinusas AJ. Effects of adenosine and a selective A2A adenosine receptor agonist on hemodynamic and thallium-201 and technetium-99m-sestaMIBI biodistribution and kinetics. JACC Cardiovasc Imaging. 2009;2:1198–208. - PubMed
-
- Johnson NP, Gould KL. Regadenoson versus dipyridamole hyperemia for cardiac PET imaging. JACC Cardiovasc Imaging. 2015;8:438–47. - PubMed
-
- Gould KL, Johnson NP, Bateman TM, Beanlands RS, Bengel FM, Bober R, Camici PG, Cerqueira MD, Chow BJ, Di Carli MF, Dorbala S, Gewirtz H, Gropler RJ, Kaufmann PA, Knaapen P, Knuuti J, Merhige ME, Rentrop KP, Ruddy TD, Schelbert HR, Schindler TH, Schwaiger M, Sdringola S, Vitarello J, Williams KA, Gordon D, Dilsizian V, Narula J. Anatomic versus physiologic assessment of coronary artery disease. Role of coronary flow reserve, fractional flow reserve, and positron emission tomography imaging in revascularization decision-making. J Am Coll Cardiol. 2013;62:1639–53. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
