

Tubulointerstitial Nephritis with IgM-Positive Plasma Cells
- PMID: 28794148
- PMCID: PMC5698061
- DOI: 10.1681/ASN.2016101074
Tubulointerstitial Nephritis with IgM-Positive Plasma Cells
Abstract
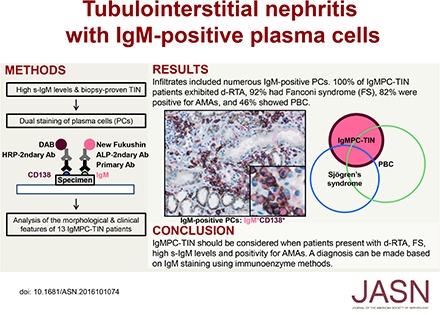
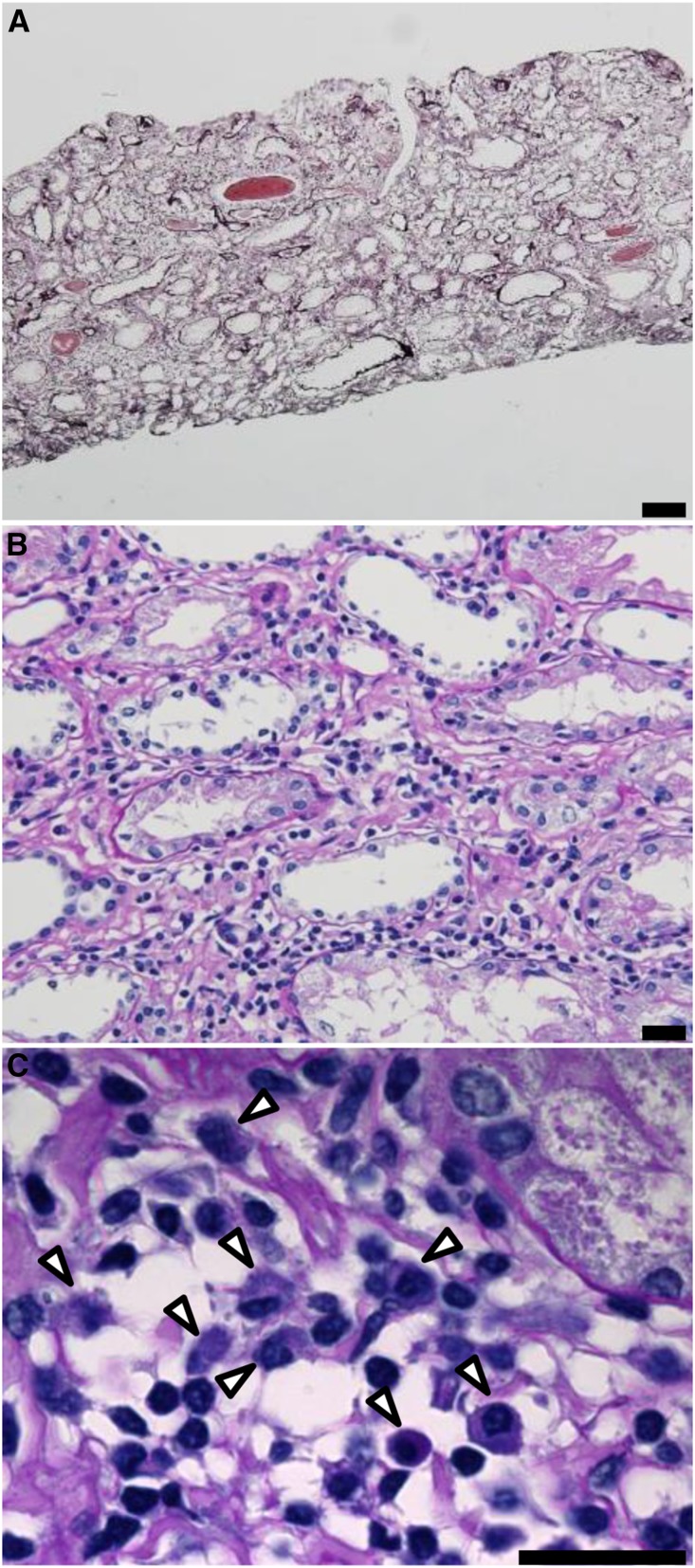
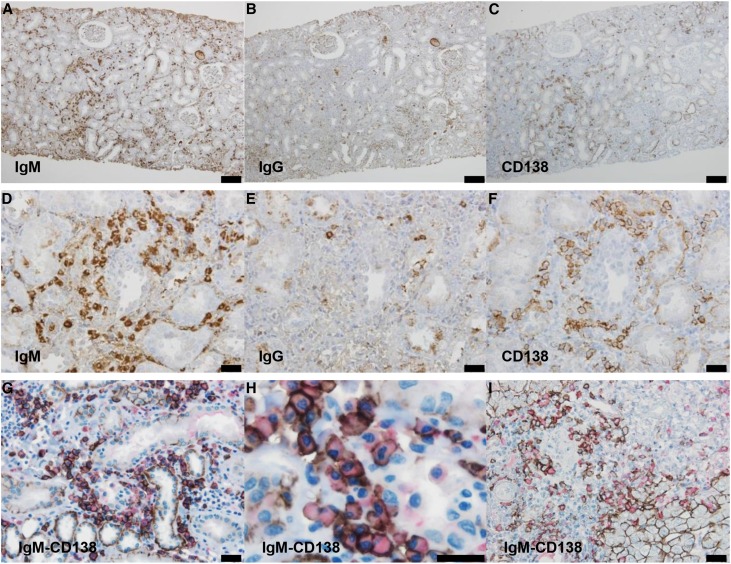
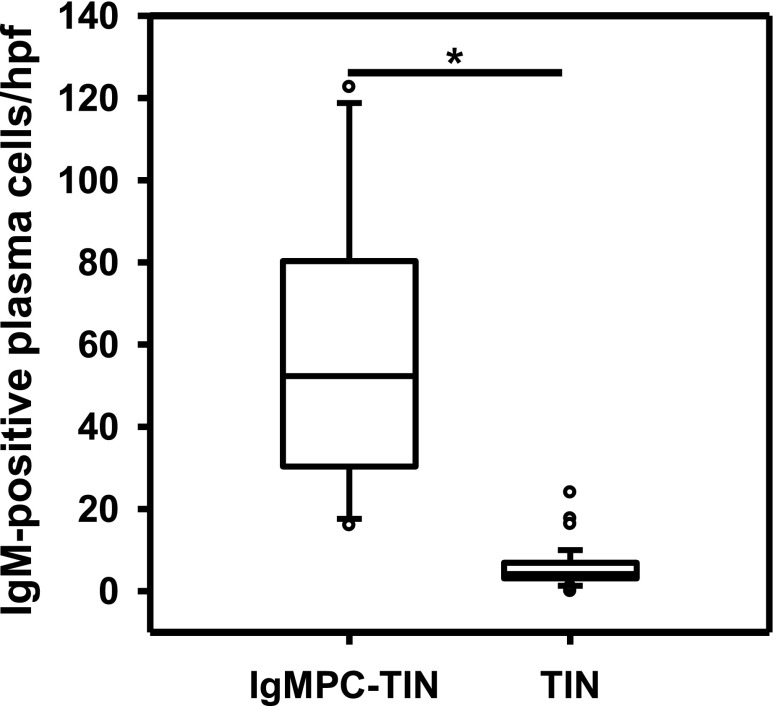
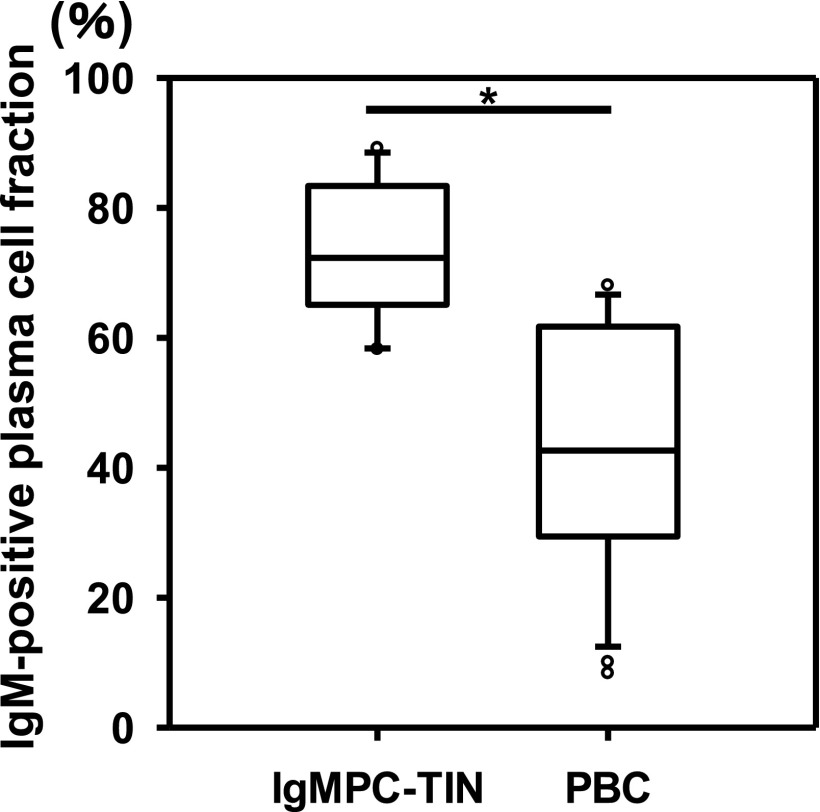
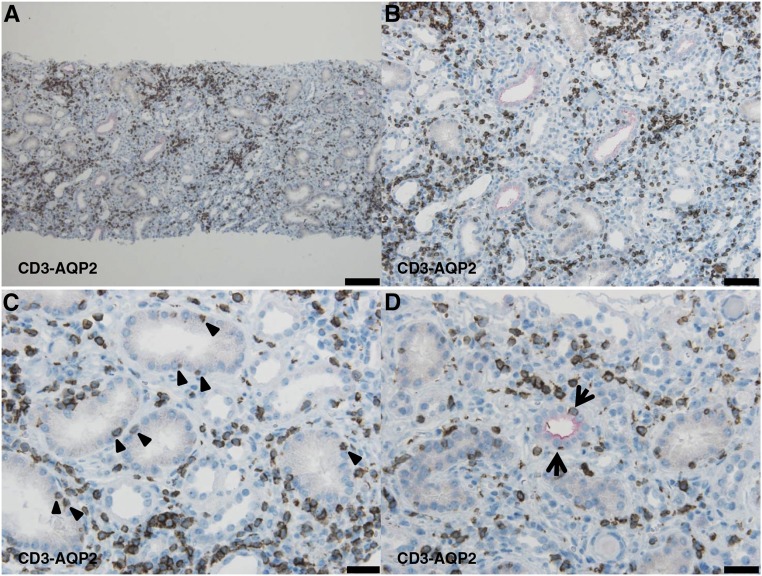
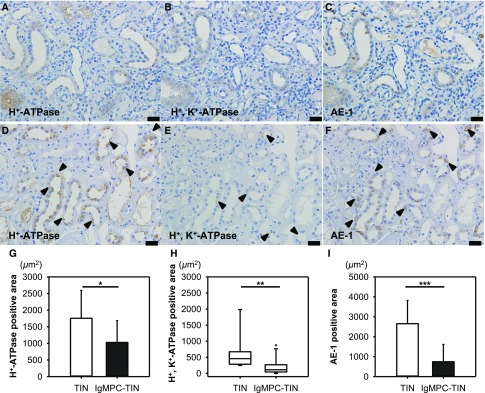
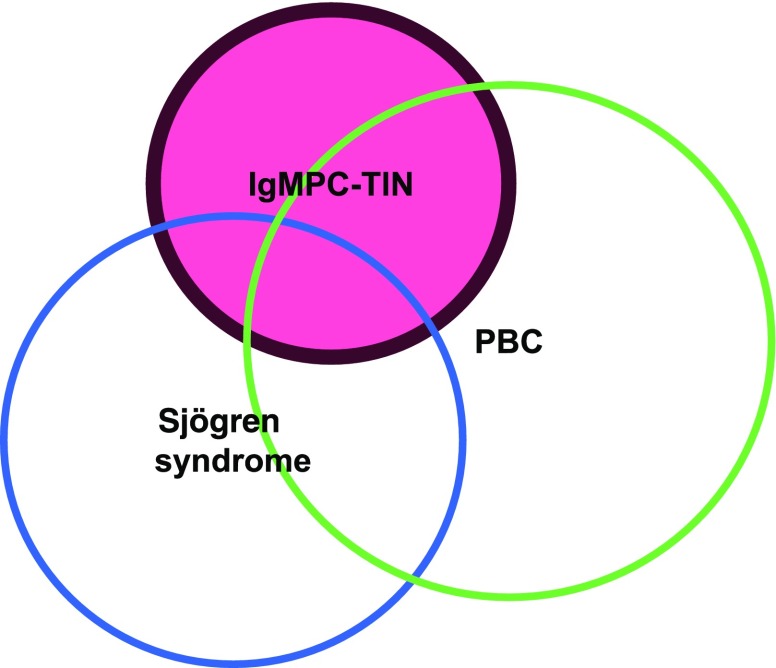
Infiltration by IgG-positive plasma cells is a common finding in tubulointerstitial nephritis. Indeed, it has been thought that CD138-positive mature plasma cells secrete mainly IgG, and the occurrence of tubulointerstitial nephritis with CD138-positive plasma cells secreting IgM has rarely been reported. Routine immunofluorescence of fresh frozen sections is considered the gold standard for detection of immune deposits. However, the immunoenzyme method with formalin-fixed, paraffin-embedded sections is superior for detecting IgM- or IgG-positive cells within the renal interstitium, thus histologic variants may often go undetected. We recently discovered a case of tubulointerstitial nephritis showing IgM-positive plasma cell accumulation within the interstitium. To further explore the morphologic and clinical features of such cases, we performed a nationwide search for patients with biopsy-proven tubulointerstitial nephritis and high serum IgM levels. We identified 13 patients with tubulointerstitial nephritis and IgM-positive plasma cell infiltration confirmed with the immunoenzyme method. The clinical findings for these patients included a high prevalence of distal renal tubular acidosis (100%), Fanconi syndrome (92%), and anti-mitochondrial antibodies (82%). The pathologic findings were interstitial nephritis with diffusely distributed CD3-positive T lymphocytes and colocalized IgM-positive plasma cells, as well as tubulitis with CD3-positive T lymphocytes in the proximal tubules and collecting ducts. Additionally, levels of H+-ATPase, H+, K+-ATPase, and the HCO3--Cl- anion exchanger were markedly decreased in the collecting ducts. We propose to designate this group of cases, which have a common histologic and clinical form, as IgM-positive plasma cell-tubulointerstitial nephritis.
Keywords: Fanconi syndrome; IgM; plasma cell; renal tubular acidosis (RTA); tubulointerstitial nephritis (TIN).
Copyright © 2017 by the American Society of Nephrology.
Figures
References
-
- Churg J, Cotran R, Sinniah R, Sakaguchi H, Sobin L: Renal Disease: Classification and Atlas of Tubulo-Interstitial Diseases, Tokyo, Igaku-Shoin, 1985
-
- Colvin R, Fang L: Interstitial nephritis. In: Renal Pathology with Clinical and Functional Correlations, edited by Tisher C, Brenner B, Philadelphia, JB Lippincott, 1994, pp 723–768
-
- Saeki T, Nishi S, Imai N, Ito T, Yamazaki H, Kawano M, Yamamoto M, Takahashi H, Matsui S, Nakada S, Origuchi T, Hirabayashi A, Homma N, Tsubata Y, Takata T, Wada Y, Saito A, Fukase S, Ishioka K, Miyazaki K, Masaki Y, Umehara H, Sugai S, Narita I: Clinicopathological characteristics of patients with IgG4-related tubulointerstitial nephritis. Kidney Int 78: 1016–1023, 2010 - PubMed
-
- Saeki T, Kawano M: IgG4-related kidney disease. Kidney Int 85: 251–257, 2014 - PubMed
-
- Takahashi N, Kimura H, Kawajiri Y, Mikami D, Yamamoto C, Kasuno K, Imai N, Kuroda T, Nishi S, Yamamoto M, Yoshida H: Tubulointerstitial nephritis with IgM-positive plasmacytoid large lymphocyte infiltration in a patient with primary biliary cirrhosis and Sjögren’s syndrome. Clin Nephrol 74: 74–80, 2010 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
