

The association of tidal EFL with exercise performance, exacerbations, and death in COPD
- PMID: 28794622
- PMCID: PMC5536237
- DOI: 10.2147/COPD.S138720
The association of tidal EFL with exercise performance, exacerbations, and death in COPD
Abstract
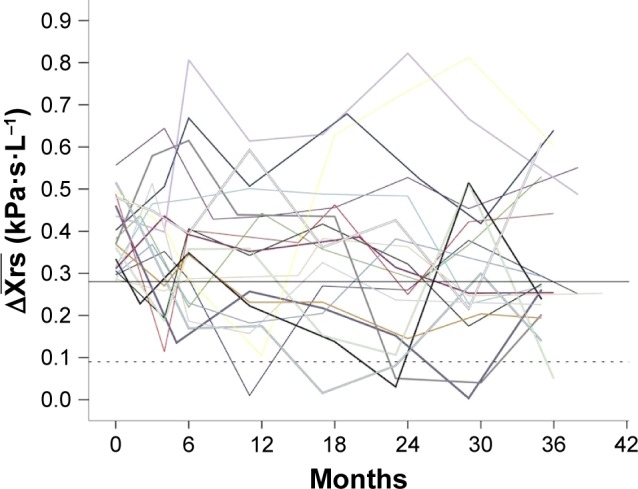
Background: Tidal expiratory flow limitation (EFLT) is frequently found in patients with COPD and can be detected by forced oscillations when within-breath reactance of a single-breath is ≥0.28 kPa·s·L-1. The present study explored the association of within-breath reactance measured over multiple breaths and EFLT with 6-minute walk distance (6MWD), exacerbations, and mortality.
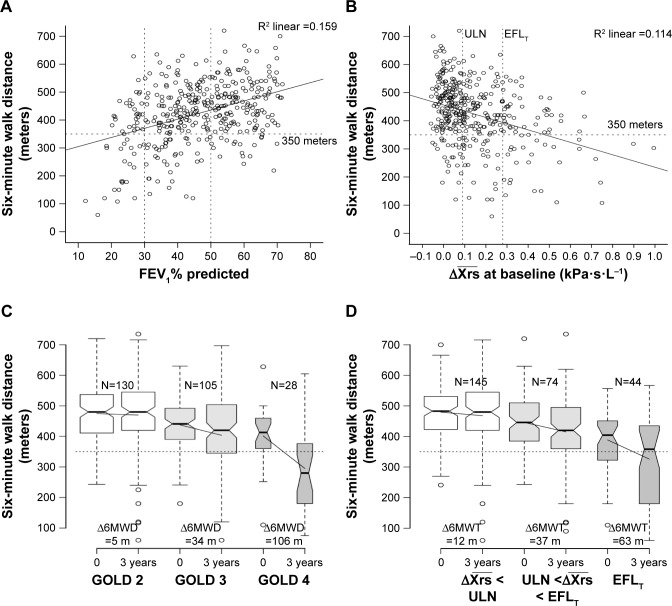
Methods: In 425 patients, spirometry and forced oscillation technique measurements were obtained on eight occasions over 3 years. 6MWD was assessed at baseline and at the 3-year visit. Respiratory symptoms, exacerbations, and hospitalizations were recorded. A total of 5-year mortality statistics were retrieved retrospectively. We grouped patients according to the mean within-breath reactance [Formula: see text], measured over several breaths at baseline, calculated as mean inspiratory-mean expiratory reactance over the sampling period. In addition to the established threshold of EFLT, an upper limit of normal (ULN) was defined using the 97.5th percentile of [Formula: see text], of the healthy controls in the study; 6MWDs were compared according to [Formula: see text], as normal, ≥ ULN < EFLT, or ≥ EFLT. Annual exacerbation rates were analyzed using a negative binomial model in the three groups, supplemented by time to first exacerbation analysis, and dichotomizing patients at the ULN.
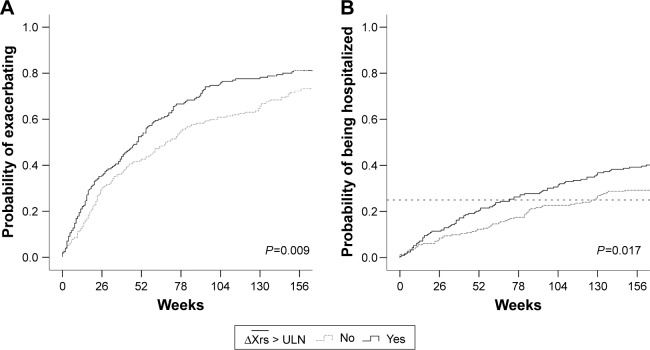
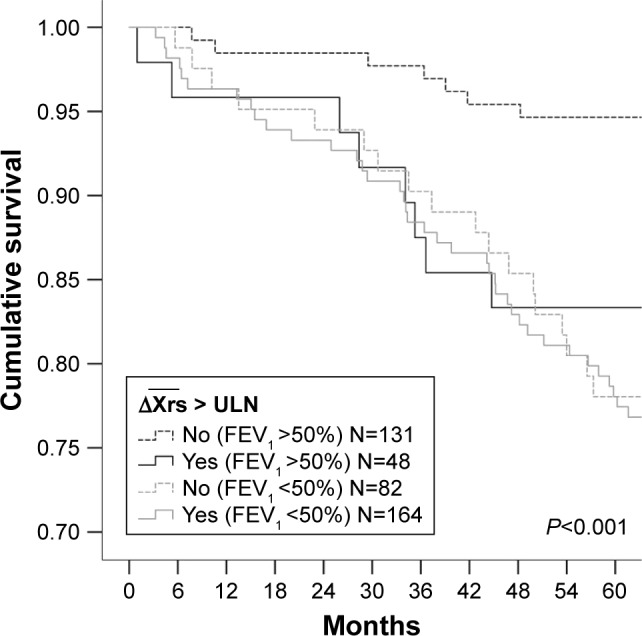
Results: In patients with COPD and baseline [Formula: see text] below the ULN (0.09 kPa·s·L-1), 6MWD was stable. 6MWD declined significantly in patients with [Formula: see text]. Worse lung function and more exacerbations were found in patients with COPD with [Formula: see text], and patients with [Formula: see text] had shorter time to first exacerbation and hospitalization. A significantly higher mortality was found in patients with [Formula: see text] and FEV1 >50%.
Conclusion: Patients with baseline [Formula: see text] had a deterioration in exercise performance, more exacerbations, and greater hospitalizations, and, among those with moderate airway obstruction, a higher mortality. [Formula: see text] is a novel independent marker of outcome in COPD.
Keywords: 6-minute walk test; COPD; exacerbations; forced oscillation technique; mortality; reactance.
Conflict of interest statement
Disclosure The authors report no conflicts of interest in this work.
Figures
References
-
- From the Global Strategy for the Diagnosis, Management and Prevention of COPD Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2017. [Accessed April 18, 2017]. Available from: http://goldcopd.org/gold-2017-global-strategy-diagnosis-management-preve...
-
- Soriano JB, Alfageme I, Almagro P, et al. Distribution and prognostic validity of the new Global Initiative for Chronic Obstructive Lung Disease grading classification. Chest. 2013;143(3):694–702. - PubMed
-
- Franciosi LG, Page CP, Celli BR, et al. Markers of disease severity in chronic obstructive pulmonary disease. Pulm Pharmacol Ther. 2006;19(3):189–199. - PubMed
-
- Gelb AF, Hogg JC, Müller NL, et al. Contribution of emphysema and small airways in COPD. Chest. 1996;109(2):353–359. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
