

Distal Musculotendinous T Junction Injuries of the Biceps Femoris: An MRI Case Review
- PMID: 28795071
- PMCID: PMC5524253
- DOI: 10.1177/2325967117714998
Distal Musculotendinous T Junction Injuries of the Biceps Femoris: An MRI Case Review
Abstract
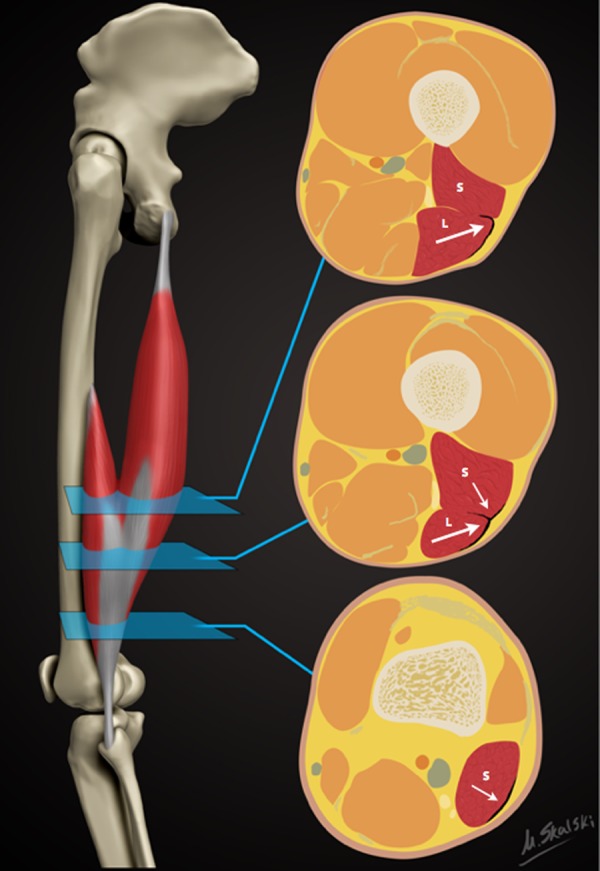
Background: Injury to the distal musculotendinous T junction (DMTJ) of the biceps femoris is a distinct clinical entity that behaves differently from other hamstring injuries due to its complex, multicomponent anatomy and dual innervation. Injury in this region demonstrates a particularly high rate of recurrence, even with prolonged rehabilitation times.
Purpose: To describe the anatomy of the DMTJ of the biceps femoris and analyze the injury patterns seen on magnetic resonance imaging (MRI) to aid prognosis and rehabilitation and minimize the risk of recurrence.
Study design: Cross-sectional study; Level of evidence, 3.
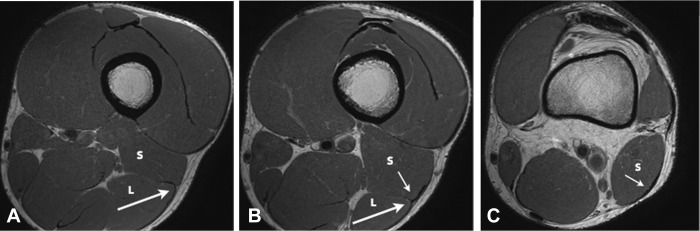
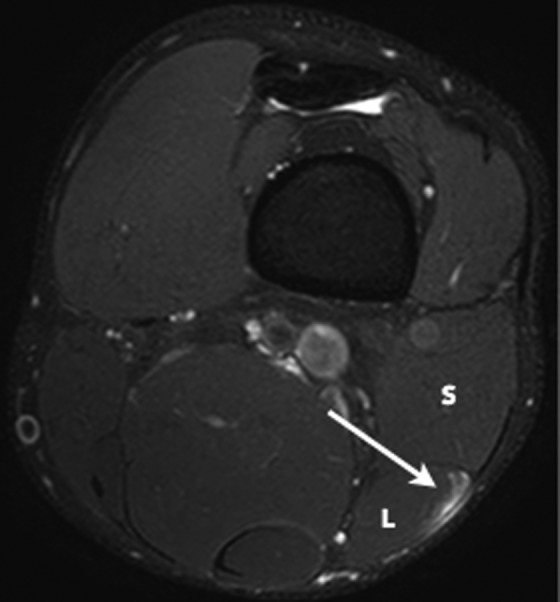
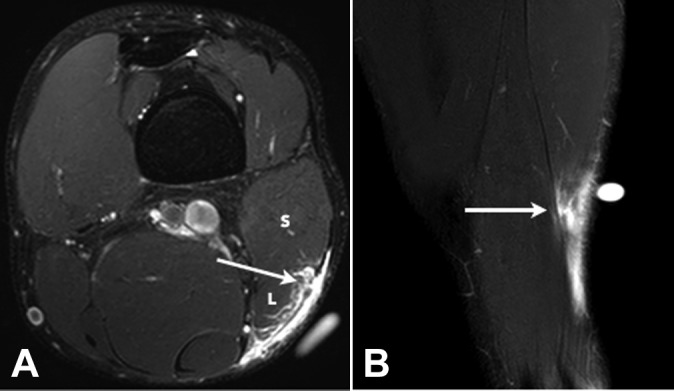
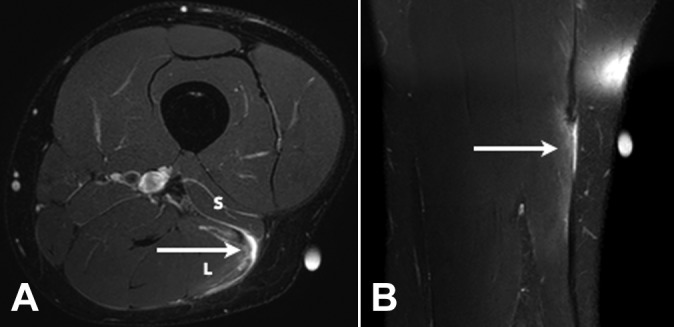
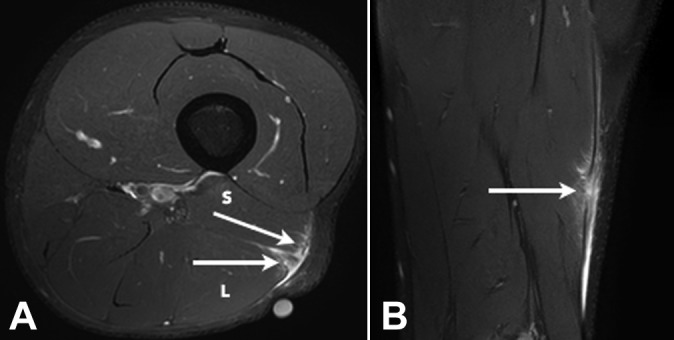
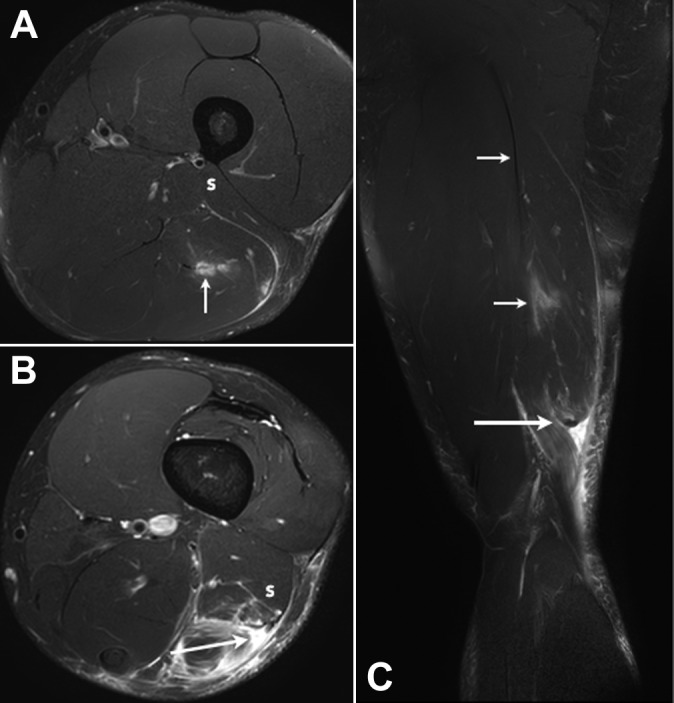
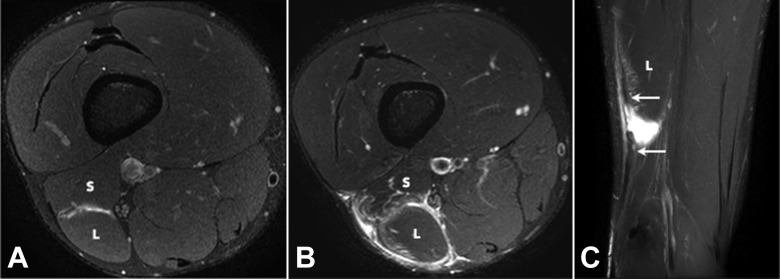
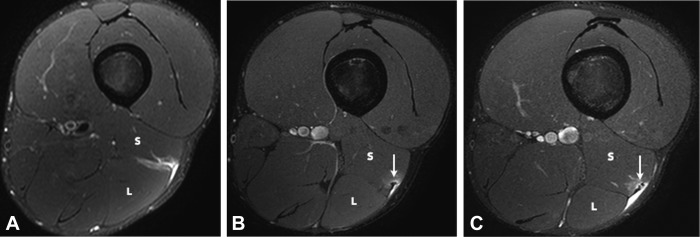
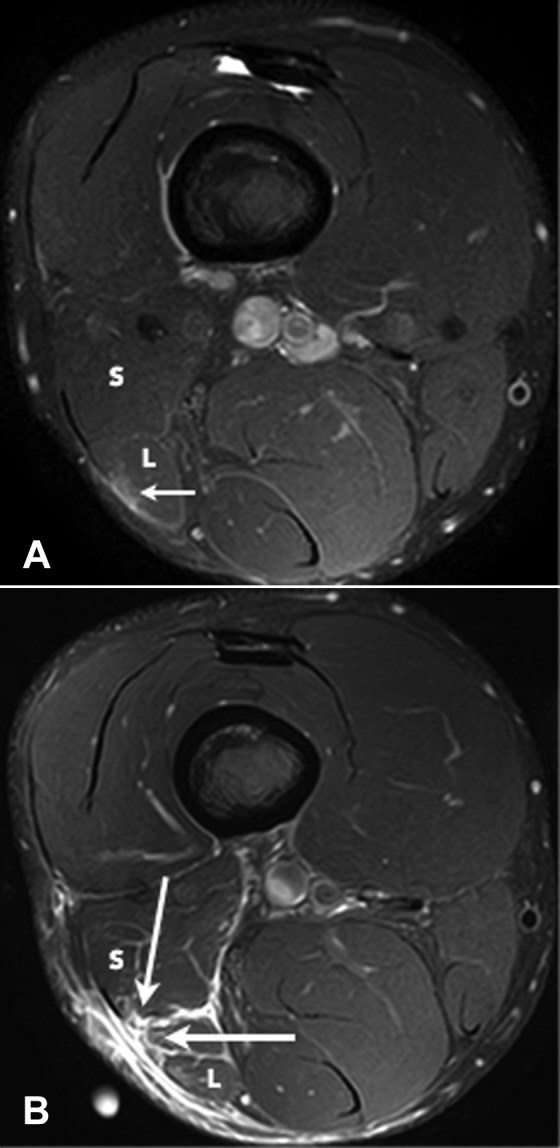
Methods: Acute injury to the DMTJ of the biceps femoris was identified in 106 MRI examinations from 55 patients at a single institution. Each injury was classified as involving the long head, the short head, or both components of the DMTJ, with each component individually graded. Injuries were classified as recurrent if there was a previous MRI demonstrating an acute injury to the DMTJ or if there was scarring present at the site of an acute injury.
Results: Of the 106 acute injuries to the DMTJ of the biceps femoris, isolated injury to the long head component was the most common (51%), with both components involved in [round 42.5% to 43%] of cases. Isolated injury to the short head component accounted for 7% of cases. The recurrence rate for reinjury to the DMTJ was 54% in this series. The date of prior injury was known in 45 of 57 recurrent cases, with 34 of these reoccurring within 3 months (76%) and 40 reoccurring within 12 months (89%). The recurrent injury was of a higher grade than the prior injury in 22 of 44 instances (50%), the same grade in 16 instances (36%), and a lower grade in 6 instances (14%). Thus, 86% of recurrent injuries were of the same or higher grade than prior injury.
Conclusion: These results suggest that high-risk muscle injuries, such as that to the DMTJ of the biceps femoris, should be evaluated using MRI to determine the structural components involved and to assess the extent and severity of injury.
Keywords: biceps femoris; hamstring; magnetic resonance imaging; muscle injury.
Conflict of interest statement
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Figures
References
-
- Ahmad CS, Redler LH, Ciccotti MG, Maffulli N, Longo UG, Bradley J. Evaluation and management of hamstring injuries. Am J Sports Med. 2013;41:2933–2947. - PubMed
-
- Arnason A, Sigurdsson SB, Gudmundsson A, Holme I, Engebretsen L, Bahr R. Risk factors for injuries in football. Am J Sports Med. 2004;32(suppl 1):5S–16S. - PubMed
-
- Brooks JH, Fuller CW, Kemp SP, Reddin DB. Incidence, risk, and prevention of hamstring muscle injuries in professional rugby union. Am J Sports Med. 2006;34:1297–1306. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
