

Metastasis-Free Survival Is a Strong Surrogate of Overall Survival in Localized Prostate Cancer
- PMID: 28796587
- PMCID: PMC5652387
- DOI: 10.1200/JCO.2017.73.9987
Metastasis-Free Survival Is a Strong Surrogate of Overall Survival in Localized Prostate Cancer
Abstract
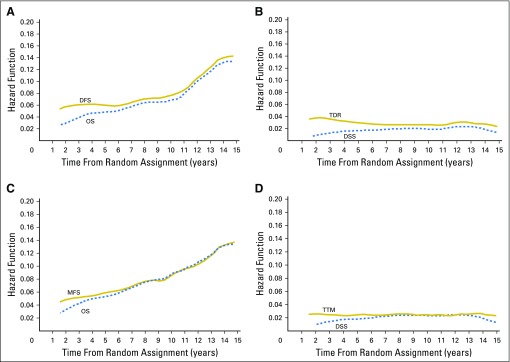
Purpose Adjuvant therapy for intermediate-risk and high-risk localized prostate cancer decreases the number of deaths from this disease. Surrogates for overall survival (OS) could expedite the evaluation of new adjuvant therapies. Methods By June 2013, 102 completed or ongoing randomized trials were identified and individual patient data were collected from 28 trials with 28,905 patients. Disease-free survival (DFS) and metastasis-free survival (MFS) were determined for 21,140 patients from 24 trials and 12,712 patients from 19 trials, respectively. We evaluated the surrogacy of DFS and MFS for OS by using a two-stage meta-analytic validation model by determining the correlation of an intermediate clinical end point with OS and the correlation of treatment effects on both the intermediate clinical end point and OS. Results Trials enrolled patients from 1987 to 2011. After a median follow-up of 10 years, 45% of 21,140 men and 45% of 12,712 men experienced a DFS and MFS event, respectively. For DFS and MFS, 61% and 90% of the patients, respectively, were from radiation trials, and 63% and 66%, respectively, had high-risk disease. At the patient level, Kendall's τ correlation with OS was 0.85 and 0.91 for DFS and MFS, respectively. At the trial level, R2 was 0.86 (95% CI, 0.78 to 0.90) and 0.83 (95% CI, 0.71 to 0.88) from weighted linear regression of 8-year OS rates versus 5-year DFS and MFS rates, respectively. Treatment effects-measured by log hazard ratios-for the surrogates and OS were well correlated ( R2, 0.73 [95% CI, 0.53 to 0.82] for DFS and 0.92 [95% CI, 0.81 to 0.95] for MFS). Conclusion MFS is a strong surrogate for OS for localized prostate cancer that is associated with a significant risk of death from prostate cancer.
Figures




Comment in
-
Surrogate Endpoint ID'd for Prostate Cancer Trials.Cancer Discov. 2017 Oct;7(10):1053-1054. doi: 10.1158/2159-8290.CD-NB2017-121. Epub 2017 Aug 29. Cancer Discov. 2017. PMID: 28851688
-
Re: Metastasis-free Survival Is a Strong Surrogate of Overall Survival in Localized Prostate Cancer.Eur Urol. 2018 Jan;73(1):141-142. doi: 10.1016/j.eururo.2017.09.033. Epub 2017 Oct 13. Eur Urol. 2018. PMID: 29033103 No abstract available.
-
Measurement of Metastasis in the Follow-Up of Localized Prostate Cancer.J Clin Oncol. 2018 Feb 10;36(5):514. doi: 10.1200/JCO.2017.76.2005. Epub 2017 Dec 21. J Clin Oncol. 2018. PMID: 29267130 No abstract available.
-
Reply to Y. Zhu et al.J Clin Oncol. 2018 Feb 10;36(5):515-516. doi: 10.1200/JCO.2017.76.2872. Epub 2017 Dec 21. J Clin Oncol. 2018. PMID: 29267131 No abstract available.
-
Surrogate end points in early prostate cancer clinical states: ready for implementation?Ann Transl Med. 2017 Dec;5(24):502. doi: 10.21037/atm.2017.10.25. Ann Transl Med. 2017. PMID: 29299463 Free PMC article. No abstract available.
-
Metastasis-Free Survival in Prostate Cancer: Faster Drug Approvals, Better Drugs?J Clin Oncol. 2019 Feb 1;37(4):266-268. doi: 10.1200/JCO.18.01092. Epub 2018 Dec 11. J Clin Oncol. 2019. PMID: 30532985 No abstract available.
References
-
- Torre LA, Bray F, Siegel RL, et al. : Global cancer statistics, 2012. CA Cancer J Clin 65:87-108, 2015 - PubMed
-
- Siegel RL, Miller KD, Jemal A: Cancer statistics, 2016. CA Cancer J Clin 66:7-30, 2016 - PubMed
-
- Bolla M, Gonzalez D, Warde P, et al. : Improved survival in patients with locally advanced prostate cancer treated with radiotherapy and goserelin. N Engl J Med 337:295-300, 1997 - PubMed
-
- Denham JW, Steigler A, Lamb DS, et al. : Short-term neoadjuvant androgen deprivation and radiotherapy for locally advanced prostate cancer: 10-year data from the TROG 96.01 randomised trial. Lancet Oncol 12:451-459, 2011 - PubMed
-
- Attard G, Parker C, Eeles RA, et al. : Prostate cancer. Lancet 387:70-82, 2016 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
