

Neonatal Morbidity of Small- and Large-for-Gestational-Age Neonates Born at Term in Uncomplicated Pregnancies
- PMID: 28796674
- PMCID: PMC5578445
- DOI: 10.1097/AOG.0000000000002199
Neonatal Morbidity of Small- and Large-for-Gestational-Age Neonates Born at Term in Uncomplicated Pregnancies
Abstract
Objective: To compare morbidity among small-for-gestational-age (SGA; birth weight less than the 10th percentile for gestational age), appropriate-for-gestational-age (AGA; birth weight 10th to 90th percentile; reference group), and large-for-gestational-age (LGA; birth weight greater than the 90th percentile) neonates in apparently uncomplicated pregnancies at term (37 weeks of gestation or greater).
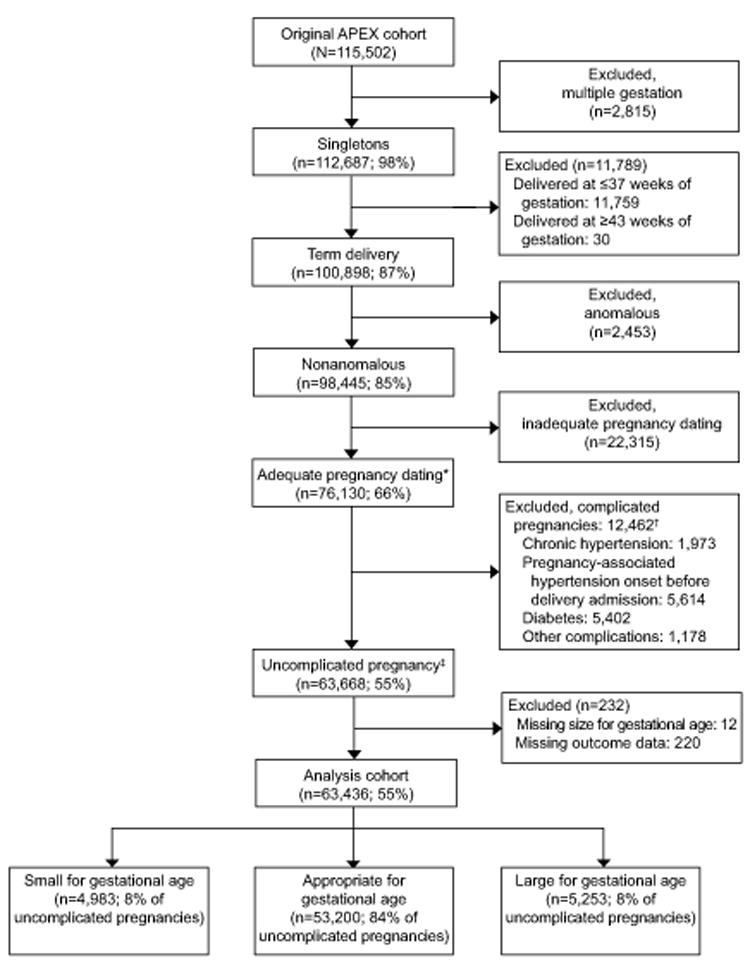
Methods: This secondary analysis, derived from an observational obstetric cohort of 115,502 deliveries, included women with apparently uncomplicated pregnancies of nonanomalous singletons who had confirmatory ultrasound dating no later than the second trimester and who delivered between 37 0/7 and 42 6/7 weeks of gestation. We used two different composite neonatal morbidity outcomes: hypoxic composite neonatal morbidity for SGA and traumatic composite neonatal morbidity for LGA neonates. Log Poisson relative risks (RRs) with 95% CIs adjusted for potential confounding factors (nulliparity, body mass index, insurance status, and neonatal sex) were calculated.
Results: Among the 63,436 women who met our inclusion criteria, SGA occurred in 7.9% (n=4,983) and LGA in 8.3% (n=5,253). Hypoxic composite neonatal morbidity was significantly higher in SGA (1.1%) compared with AGA (0.7%; adjusted RR 1.44, 95% CI 1.07-1.93) but similar between LGA (0.6%) and AGA (adjusted RR 0.84, 95% CI 0.58-1.22). Traumatic composite neonatal morbidity was significantly higher in LGA (1.9%) than AGA (1.0%; adjusted RR 1.88, 95% CI 1.51-2.34) but similar in SGA (1.3%) compared with AGA (adjusted RR 1.28, 95% CI 0.98-1.67).
Conclusion: Among women with uncomplicated pregnancies, hypoxic composite neonatal morbidity is more common with SGA neonates and traumatic-composite neonatal morbidity is more common with LGA neonates.
Conflict of interest statement
The authors did not report any potential conflicts of interest.
Figures
References
-
- Chen HY, Chauhan SP, Ward TC, Mori N, Gass ET, Cisler RA. Aberrant fetal growth and early, late, and postneonatal mortality: an analysis of Milwaukee births 1996-2007. Am J Obstet Gynecol. 2011;204(261):e1–261. e10. - PubMed
-
- American College of Obstetricians and Gynecologists. ACOG Practice Bulletin No 134. Washington DC: ACOG; 2013. Fetal growth restriction.
-
- American College of Obstetricians and Gynecologists. ACOG Practice Bulletin No 173. Washington DC: ACOG; 2016. Fetal macrosomia.
-
- Sibai BM, Abdella TN, Anderson GD. Pregnancy outcome in 211 patients with mild chronic hypertension. Obstet Gynecol. 1983;61:571–6. - PubMed
Publication types
MeSH terms
Grants and funding
- U10 HD040500/HD/NICHD NIH HHS/United States
- UG1 HD027869/HD/NICHD NIH HHS/United States
- U10 HD040544/HD/NICHD NIH HHS/United States
- UG1 HD040560/HD/NICHD NIH HHS/United States
- UG1 HD087230/HD/NICHD NIH HHS/United States
- UG1 HD053097/HD/NICHD NIH HHS/United States
- UG1 HD027915/HD/NICHD NIH HHS/United States
- U10 HD040485/HD/NICHD NIH HHS/United States
- U10 HD034116/HD/NICHD NIH HHS/United States
- U10 HD027869/HD/NICHD NIH HHS/United States
- U10 HD027917/HD/NICHD NIH HHS/United States
- UL1 TR000439/TR/NCATS NIH HHS/United States
- UG1 HD040485/HD/NICHD NIH HHS/United States
- U10 HD040560/HD/NICHD NIH HHS/United States
- UG1 HD040500/HD/NICHD NIH HHS/United States
- U10 HD040512/HD/NICHD NIH HHS/United States
- U10 HD040545/HD/NICHD NIH HHS/United States
- U01 HD036801/HD/NICHD NIH HHS/United States
- U10 HD053118/HD/NICHD NIH HHS/United States
- UL1 RR024989/RR/NCRR NIH HHS/United States
- UL1 RR025764/RR/NCRR NIH HHS/United States
- UG1 HD034116/HD/NICHD NIH HHS/United States
- UG1 HD040544/HD/NICHD NIH HHS/United States
- UG1 HD034208/HD/NICHD NIH HHS/United States
- UG1 HD040512/HD/NICHD NIH HHS/United States
- U10 HD027915/HD/NICHD NIH HHS/United States
- UG1 HD040545/HD/NICHD NIH HHS/United States
- U10 HD034208/HD/NICHD NIH HHS/United States
- U10 HD053097/HD/NICHD NIH HHS/United States
- P2C HD050924/HD/NICHD NIH HHS/United States
- U10 HD021410/HD/NICHD NIH HHS/United States
- U10 HD036801/HD/NICHD NIH HHS/United States
- U24 HD036801/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
