

Postoperative Chemoradiotherapy After Local Resection for High-Risk T1 to T2 Low Rectal Cancer: Results of a Single-Arm, Multi-Institutional, Phase II Clinical Trial
- PMID: 28796729
- PMCID: PMC5553237
- DOI: 10.1097/DCR.0000000000000870
Postoperative Chemoradiotherapy After Local Resection for High-Risk T1 to T2 Low Rectal Cancer: Results of a Single-Arm, Multi-Institutional, Phase II Clinical Trial
Abstract
Background: After treatment with local excision for TNM stage I low rectal cancer, the risk of local recurrence is not only high for T2 lesions but also for T1 lesions with features of massive invasion to the submucosal layer and/or lymphovascular invasion.
Objective: The purpose of this study was to determine the efficacy of chemoradiotherapy combined with local excision in the treatment of T1 to T2 low rectal cancer.
Design: We conducted a prospective, single-arm, phase II trial.
Settings: This was a multicenter study.
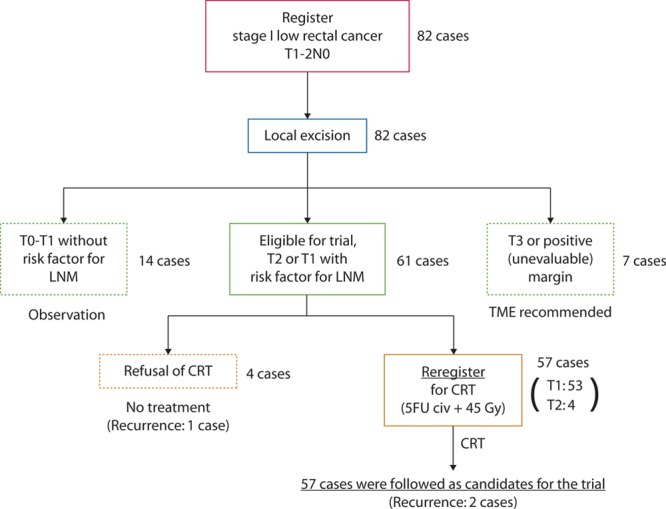
Patients: From April 2003 to October 2010, 57 patients were treated with local excision after additional external beam irradiation (45 Gy) plus continuous 5-week intravenous injection of 5-fluorouracil (250 mg/m per day) at 10 domestic hospitals. Fifty-three patients had clinical T1N0 lesions, and 4 had T2N0 lesions in the low rectum, located below the peritoneal reflection.
Main outcomes measures: The primary end point was disease-free survival at 5 years.
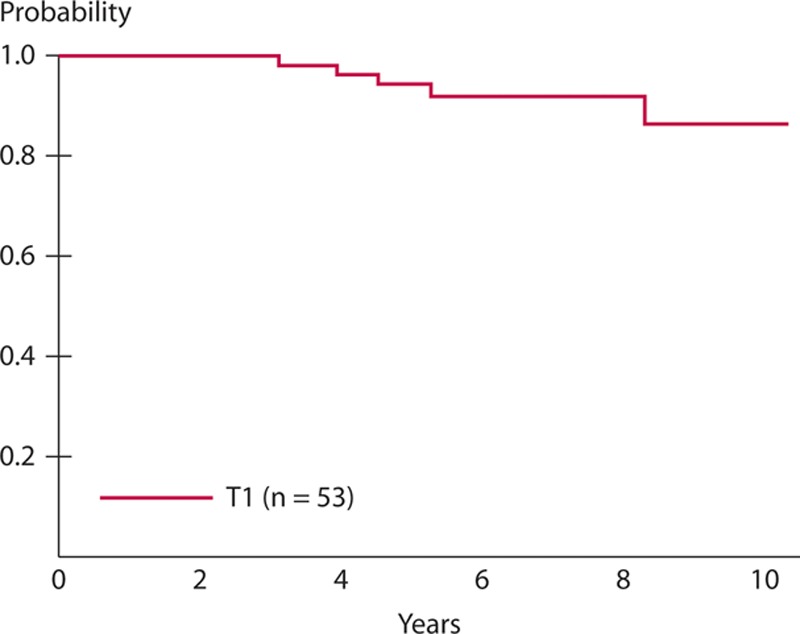
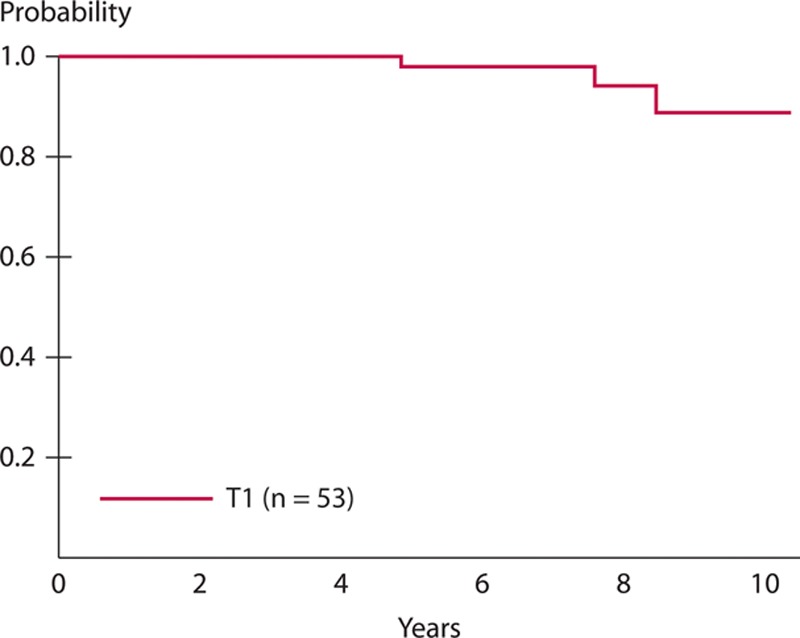
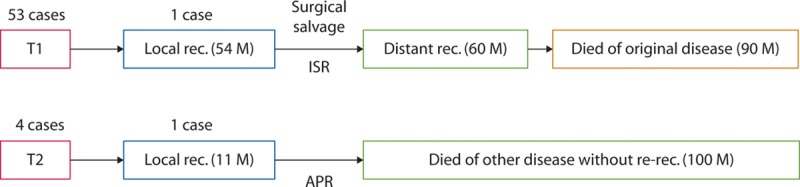
Results: The completion rate for full-dose chemoradiotherapy was 86% (49/57). Serious, nontransient treatment-related complications were not reported. With a median follow-up of 7.3 years after local excision, the 5-year disease-free survival rate was 94% for the 53 patients with T1 lesions and 75% for the 4 patients with T2 lesions. There were 2 local recurrences during the entire observation period. Anal function after local excision and chemoradiation were kept at almost the same levels as observed before treatment.
Limitations: The study was limited by the small number of registered T2 rectal cancers, retrospective evaluations of quality of life, and the exclusion of poorly differentiated adenocarcinoma (a high-risk feature of T1 lesions).
Conclusions: The addition of chemoradiotherapy to local excision of T1 rectal adenocarcinomas with poor prognostic features including deep submucosal invasion and lymphovascular invasion could improve on less favorable historic oncologic outcomes of local excision alone in this high-risk group for lymph node metastasis. See Video Abstract at http://links.lww.com/DCR/A421.
Conflict of interest statement
Figures
References
-
- Hager T, Gall FP, Hermanek P.Local excision of cancer of the rectum. Dis Colon Rectum. 1983;26:149–151. - PubMed
-
- Stearns MW, Jr, Sternberg SS, DeCosse JJ.Treatment alternatives: localized rectal cancer. Cancer. 1984;54(11 suppl):2691–2694. - PubMed
-
- Whiteway J, Nicholls RJ, Morson BC.The role of surgical local excision in the treatment of rectal cancer. Br J Surg. 1985;72:694–697. - PubMed
-
- Biggers OR, Beart RW, Jr, Ilstrup DM.Local excision of rectal cancer. Dis Colon Rectum. 1986;29:374–377. - PubMed
-
- Billingham RP.Conservative treatment of rectal cancer: extending the indications. Cancer. 1992;70(5 suppl):1355–1363. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
