

Phlebotomine sand fly-borne pathogens in the Mediterranean Basin: Human leishmaniasis and phlebovirus infections
- PMID: 28796786
- PMCID: PMC5552025
- DOI: 10.1371/journal.pntd.0005660
Phlebotomine sand fly-borne pathogens in the Mediterranean Basin: Human leishmaniasis and phlebovirus infections
Abstract
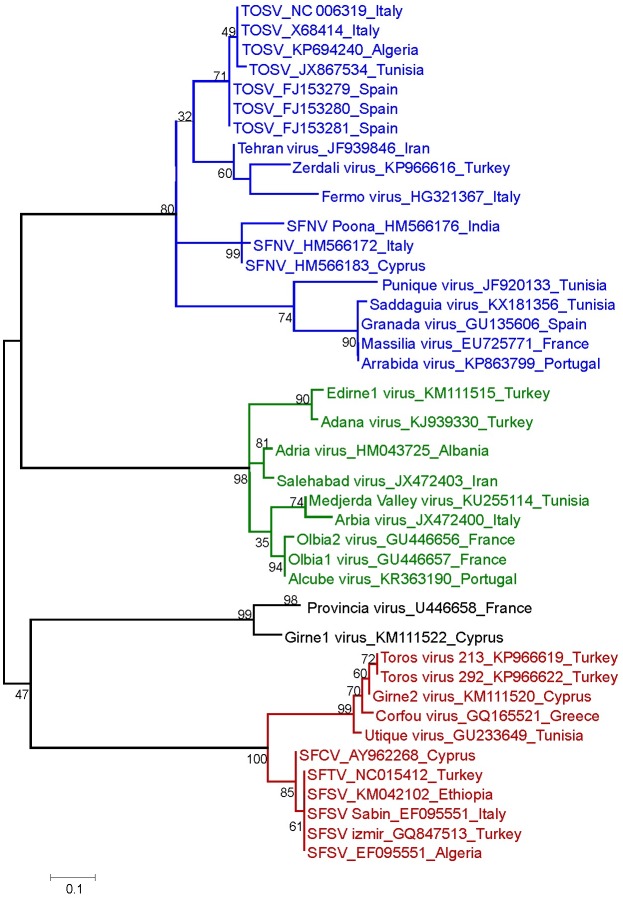
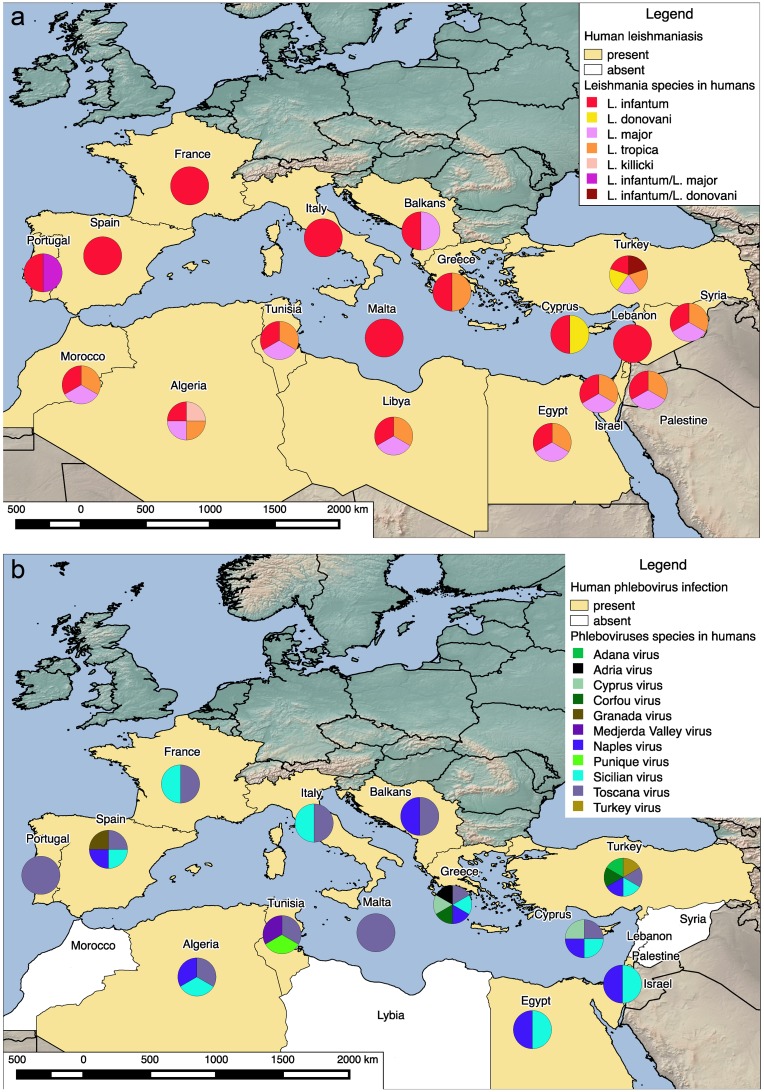
Pathogens transmitted to humans by phlebotomine sand flies are neglected, as they cause infectious diseases that are not on the priority list of national and international public health systems. However, the infections caused by protozoa of the Leishmania genus and viruses belonging to the Phlebovirus genus (family Phenuiviridae)-the most significant group of viruses transmitted by sand flies-have a relevant role for human pathology. These infections are emerging in the Mediterranean region and will likely spread in forthcoming decades, posing a complex threat to human health. Four species and 2 hybrid strains of Leishmania are pathogenic for humans in the Mediterranean Basin, with an estimated annual incidence of 239,500-393,600 cases of cutaneous leishmaniasis and 1,200-2,000 cases of visceral leishmaniasis. Among the phleboviruses, Toscana virus can cause neuroinvasive infections, while other phleboviruses are responsible for a typical "3-day fever"; the actual incidence of Phlebovirus infections in the Mediterranean area is unknown, although at least 250 million people are exposed. Here, we reviewed the current literature on epidemiology of sand fly-borne infections in the Mediterranean Basin, with a focus on humans. Our analysis indicates the need for increased public health activities directed to determine the disease burden of these infections as well as to improve their surveillance. Among the emerging challenges concerning sand fly-borne pathogens, the relationships between sand fly-borne protozoa and viruses should be considered in future studies, including epidemiological links between Leishmania and phleboviruses as well as the conditional capacity for these pathogens to be involved in interactions that may evolve towards increased virulence.
Conflict of interest statement
The authors have declared that no competing interest exist.
Figures
References
-
- Dujardin JC, Campino L, Cañavate C, Dedet JP, Gradoni L, Soteriadou K, et al. Spread of vector-borne diseases and neglect of Leishmaniasis, Europe. Emerg Infect Dis. 2008;14(7):1013–8. doi: 10.3201/eid1407.071589 - DOI - PMC - PubMed
-
- Alvar J, Vélez ID, Bern C, Herrero M, Desjeux P, Cano J, et al. Leishmaniasis worldwide and global estimates of its incidence. PLoS ONE. 2012;7(5):e35671 doi: 10.1371/journal.pone.0035671 - DOI - PMC - PubMed
-
- Alkan C, Bichaud L, de Lamballerie X, Alten B, Gould EA, Charrel RN. Sandfly-borne phleboviruses of Eurasia and Africa: epidemiology, genetic diversity, geographic range, control measures. Antiviral Res. 2013;100(1):54–74. doi: 10.1016/j.antiviral.2013.07.005 - DOI - PubMed
-
- WHO. Control of the leishmaniases: report of a meeting of the WHO Expert Committee on the Control of Leishmaniases, Geneva, 22–26 March 2010. 2010.
-
- Van der Auwera G, Dujardin JC. Species typing in dermal leishmaniasis. Clin Microbiol Rev. 2015;28(2):265–94. doi: 10.1128/CMR.00104-14 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
