

Therapeutic response assessment using 3D ultrasound for hepatic metastasis from colorectal cancer: Application of a personalized, 3D-printed tumor model using CT images
- PMID: 28797089
- PMCID: PMC5552302
- DOI: 10.1371/journal.pone.0182596
Therapeutic response assessment using 3D ultrasound for hepatic metastasis from colorectal cancer: Application of a personalized, 3D-printed tumor model using CT images
Abstract
Background & aims: To evaluate accuracy and reliability of three-dimensional ultrasound (3D US) for response evaluation of hepatic metastasis from colorectal cancer (CRC) using a personalized 3D-printed tumor model.
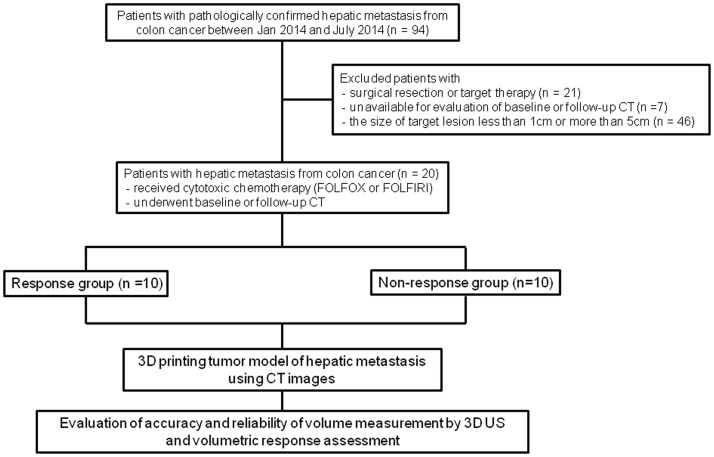
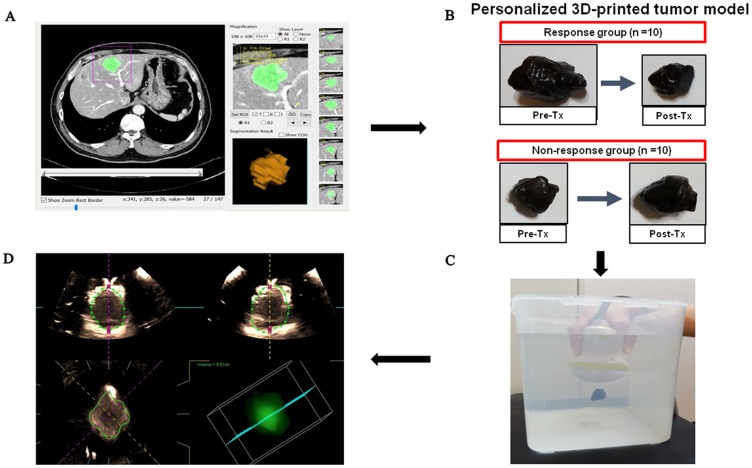
Methods: Twenty patients with liver metastasis from CRC who underwent baseline and after chemotherapy CT, were retrospectively included. Personalized 3D-printed tumor models using CT were fabricated. Two radiologists measured volume of each 3D printing model using 3D US. With CT as a reference, we compared difference between CT and US tumor volume. The response evaluation was based on Response Evaluation Criteria in Solid Tumors (RECIST) criteria.
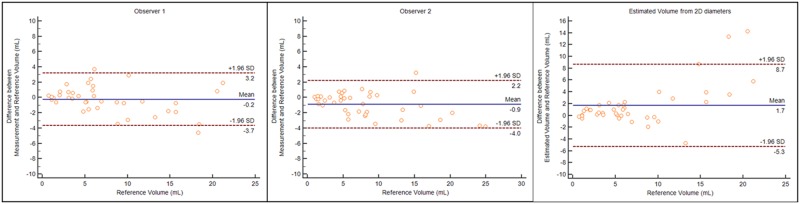
Results: 3D US tumor volume showed no significant difference from CT volume (7.18 ± 5.44 mL, 8.31 ± 6.32 mL vs 7.42 ± 5.76 mL in CT, p>0.05). 3D US provided a high correlation coefficient with CT (r = 0.953, r = 0.97) as well as a high inter-observer intraclass correlation (0.978; 0.958-0.988). Regarding response, 3D US was in agreement with CT in 17 and 18 out of 20 patients for observer 1 and 2 with excellent agreement (κ = 0.961).
Conclusions: 3D US tumor volume using a personalized 3D-printed model is an accurate and reliable method for the response evaluation in comparison with CT tumor volume.
Conflict of interest statement
Figures
References
-
- Chung W-S, Park M-S, Shin SJ, Baek S-E, Kim Y-E, Choi JY, et al. Response evaluation in patients with colorectal liver metastases: RECIST version 1.1 versus modified CT criteria. American Journal of Roentgenology. 2012;199(4):809–15. doi: 10.2214/AJR.11.7910 - DOI - PubMed
-
- Van Cutsem E, Nordlinger B, Cervantes A, Group EGW. Advanced colorectal cancer: ESMO Clinical Practice Guidelines for treatment. Annals of Oncology. 2010;21(suppl 5):v93–v7. - PubMed
-
- Fang W, Lam K, Ng S, Choi C, Kwong D, Zheng S, et al. Manual contouring based volumetric evaluation for colorectal cancer with liver limited metastases: a comparison with RECIST. Asian Pacific Journal of Cancer Prevention. 2013;14(7):4151–5. - PubMed
-
- Eisenhauer E, Therasse P, Bogaerts J, Schwartz L, Sargent D, Ford R, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). European journal of cancer. 2009;45(2):228–47. doi: 10.1016/j.ejca.2008.10.026 - DOI - PubMed
-
- Tran LN, Brown MS, Goldin JG, Yan X, Pais RC, McNitt-Gray MF, et al. Comparison of treatment response classifications between unidimensional, bidimensional, and volumetric measurements of metastatic lung lesions on chest computed tomography 1. Academic radiology. 2004;11(12):1355–60. doi: 10.1016/j.acra.2004.09.004 - DOI - PubMed
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
