

A novel whole-bacterial enzyme linked-immunosorbant assay to quantify Chlamydia trachomatis specific antibodies reveals distinct differences between systemic and genital compartments
- PMID: 28797112
- PMCID: PMC5552291
- DOI: 10.1371/journal.pone.0183101
A novel whole-bacterial enzyme linked-immunosorbant assay to quantify Chlamydia trachomatis specific antibodies reveals distinct differences between systemic and genital compartments
Abstract
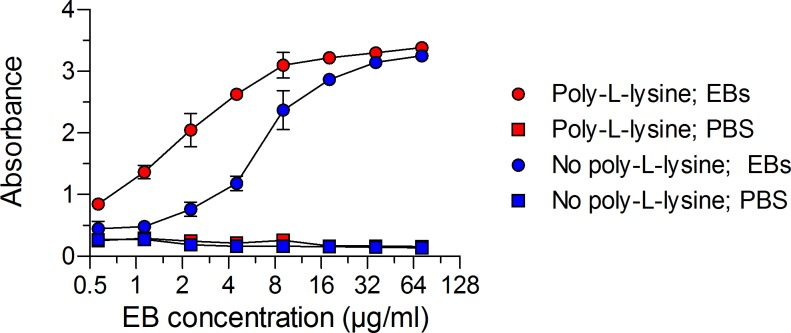
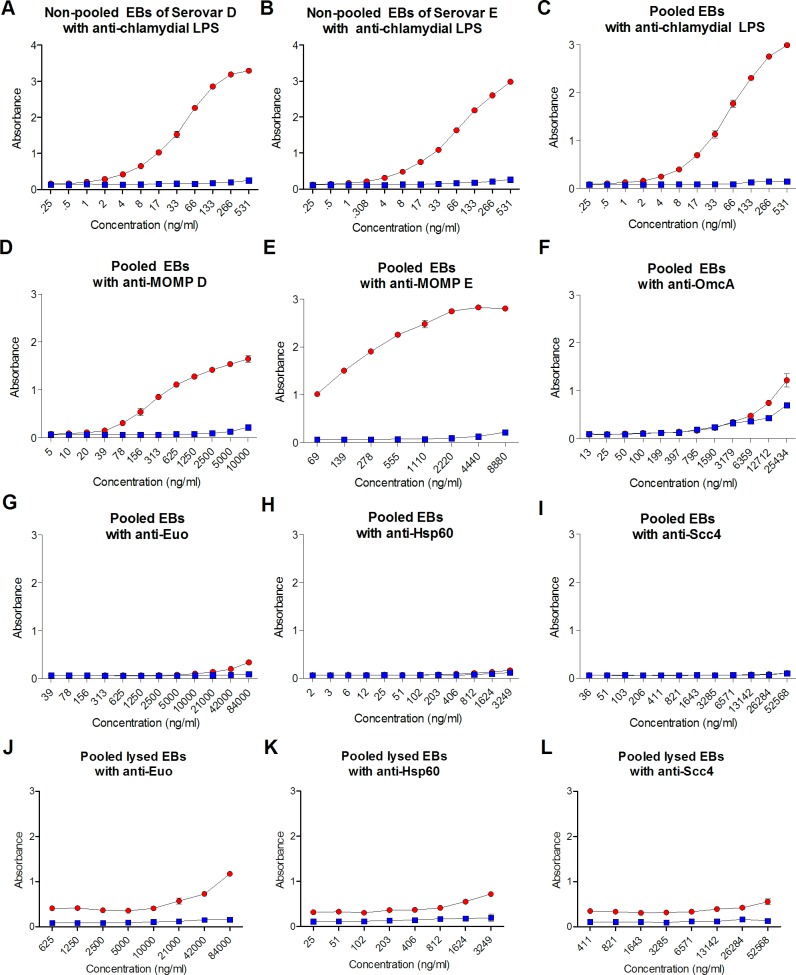
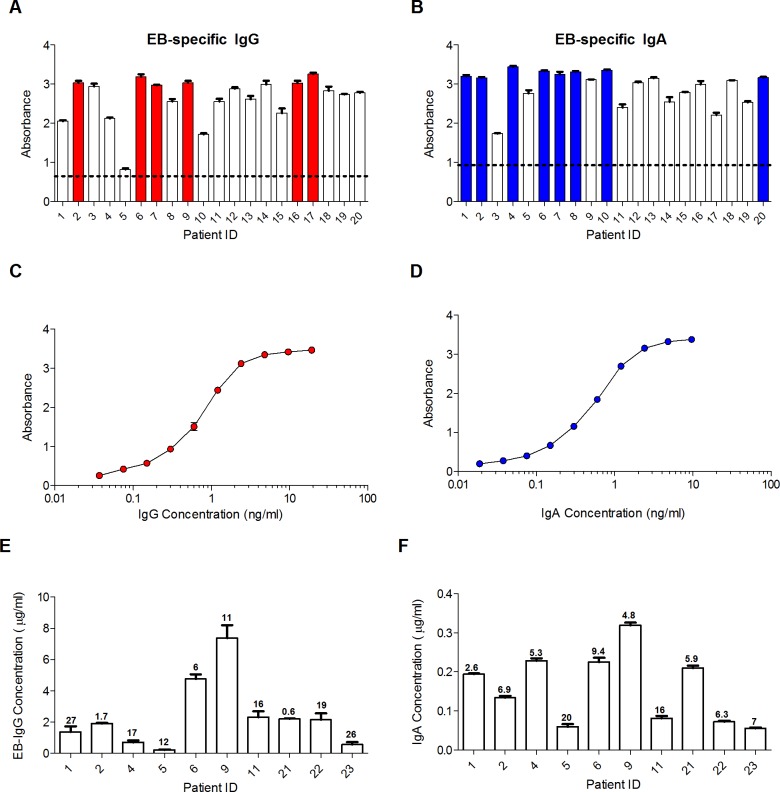
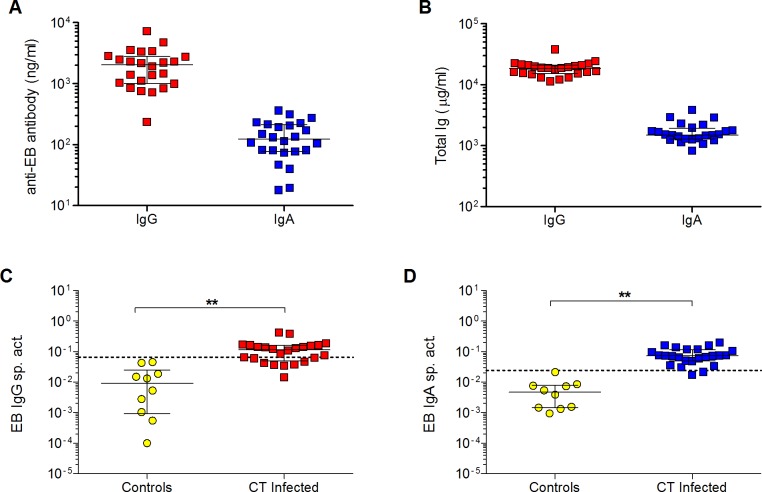
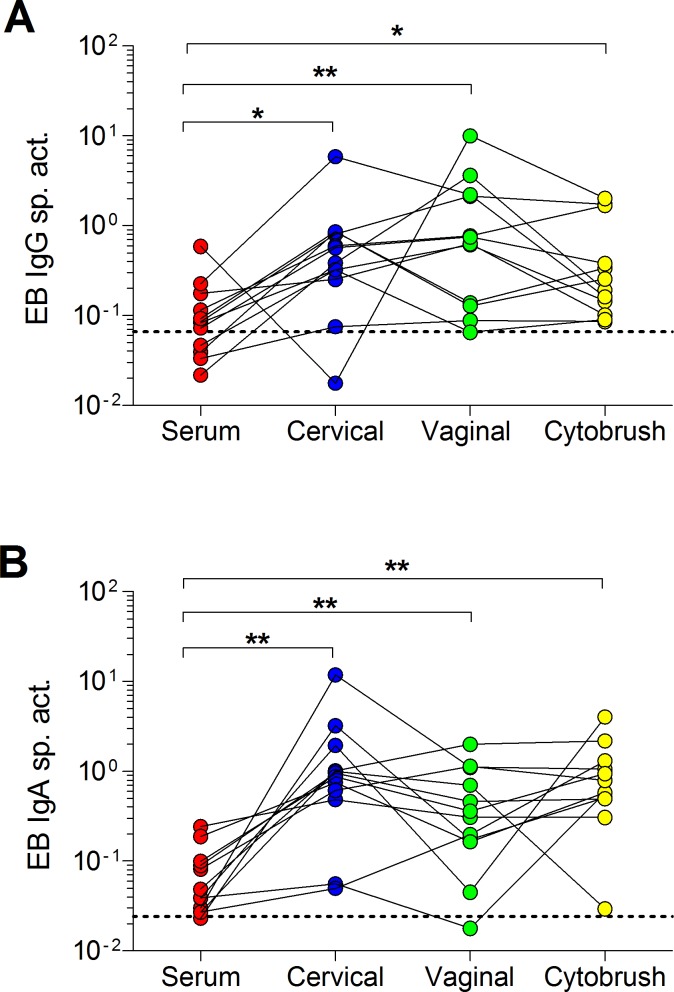
Chlamydia trachomatis (CT) is the leading sexually transmitted bacterial infection. The continued global burden of CT infection strongly predicates the need for a vaccine to supplement current chlamydial control programs. The correlates of protection against CT are currently unknown, but they must be carefully defined to guide vaccine design. The localized nature of chlamydial infection in columnar epithelial cells of the genital tract necessitates investigation of immunity at the site of infection. The purpose of this study was to develop a sensitive whole bacterial enzyme-linked immunosorbent assay (ELISA) to quantify and compare CT-specific IgG and IgA in sera and genital secretions from CT-infected women. To achieve this, elementary bodies (EBs) from two of the most common genital serovars (D and E) were attached to poly-L-lysine-coated microtiter plates with glutaraldehyde. EB attachment and integrity were verified by the presence of outer membrane antigens and the absence of bacterial cytoplasmic antigens. EB-specific IgG and IgA standards were developed by pooling sera with high titers of CT-specific antibodies from infected women. Serum, endocervical and vaginal secretions, and endocervical cytobrush specimens from CT-infected women were used to quantify CT-specific IgG and IgA which were then normalized to total IgG and IgA, respectively. Analyses of paired serum and genital samples revealed significantly higher proportions of EB-specific antibodies in genital secretions compared to sera. Cervical and vaginal secretions and cytobrush specimens had similar proportions of EB-specific antibodies, suggesting any one of these genital sampling techniques could be used to quantify CT-specific antibodies when appropriate normalization methodologies are implemented. Overall, these results illustrate the need to investigate genital tract CT antibody responses, and our assay provides a useful quantitative tool to assess natural immunity in defined clinical groups and CT vaccine trials.
Conflict of interest statement
Figures
References
-
- Peipert JF. Genital chlamydial infections. N Engl J Med. 2003;349:2424–30. doi: 10.1056/NEJMcp030542 - DOI - PubMed
-
- Golden MR, Schillinger JA, Markowitz LE, Louis ME. Duration of untreated genital infections with Chlamydia trachomatis: A review of the literature. Sex Transm Dis. 2000;27(6):329–37. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
