

Prognostic significance of BRAF and NRAS mutations in melanoma: a German study from routine care
- PMID: 28797232
- PMCID: PMC5553744
- DOI: 10.1186/s12885-017-3529-5
Prognostic significance of BRAF and NRAS mutations in melanoma: a German study from routine care
Abstract
Background: Hotspot mutations of the oncogenes BRAF and NRAS are the most common genetic alterations in cutaneous melanoma. Specific inhibitors of BRAF and MEK have shown significant survival benefits in large phase III trials. However, the prognostic significance of BRAF and NRAS mutations outside of clinical trials remains unclear.
Methods: The mutational status of BRAF (exon 15) and NRAS (exon 2 and 3) was determined in melanoma samples of 217 patients with pyrosequencing and Sanger sequencing. The genotypes were correlated with clinical outcomes and pathologic features of the primary tumors. Time to disease progression was calculated with the cumulative incidence function. Survival analyses were performed with Kaplan-Meier estimates and Cox proportional hazards regression analysis. Relative survival was calculated with the Ederer-II method. Treatment with BRAF and MEK inhibitors and immune checkpoint blockade (ICB) was allowed.
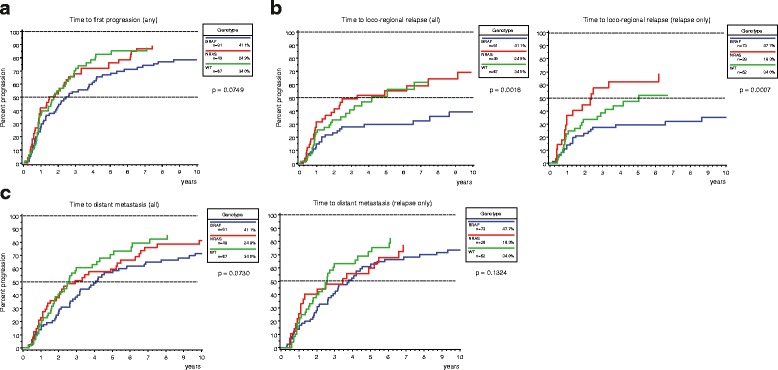
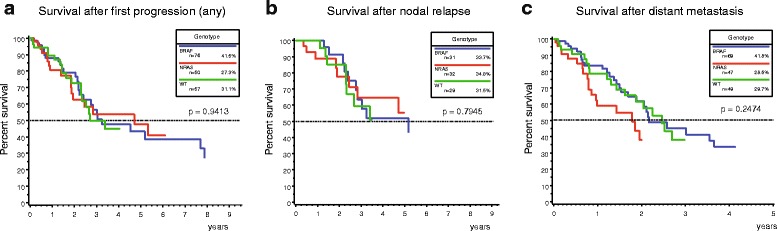
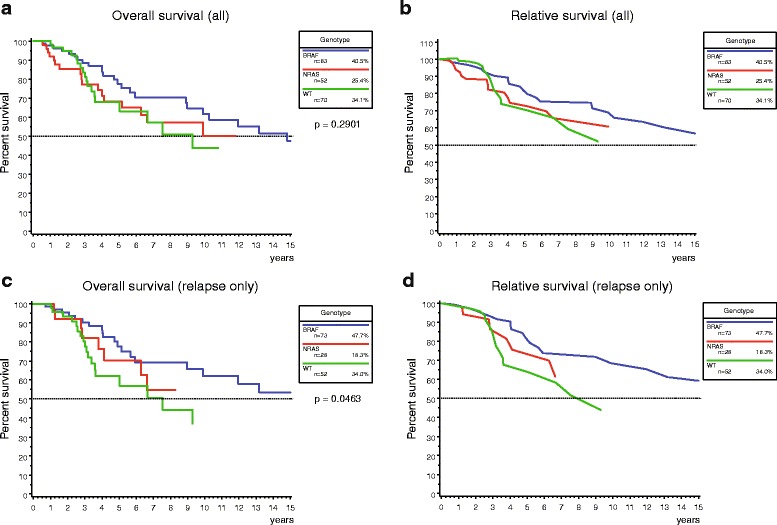
Results: Mutations in BRAF and NRAS were identified in 40.1 and 24.4% of cases, respectively. Concurrent mutations in both genes were detected in further 2.3%. The remaining 33.2% were wild type for the investigated exons (WT). BRAF mutations were significantly associated with younger age at first diagnosis (p < 0.001) and truncal localization of the culprit primary (p = 0.002). The nodular subtype was most common in the NRAS cohort. In addition, NRAS-mutant melanoma patients showed a higher frequency of nodal relapse (p = 0.013) and development of metastatic disease (p = 0.021). The time to loco-regional nodal relapse was shortest in NRAS-mutant melanoma (p = 0.002). Presence of NRAS mutation was an independent risk factor for disease progression in multivariate analysis (HR 2.01; 95% CI 1.02 - 3.98). BRAF-mutant melanoma patients showed a tendency for better overall and relative survival. Genotype was not a consistent risk factor in multivariate analysis. Instead, positive sentinel lymph node status (HR 2.65; 95% CI 1.15 - 6.10) and treatment with ICB in stage IV disease (HR 0.17; 95% CI 0.06-0.48) were significant multivariate risk factors.
Conclusions: NRAS-mutant tumors tended to behave more aggressively particularly in early stages of the disease in this high-risk melanoma population. Treatment with immune checkpoint blockade improved survival in stage IV disease in a real-world setting.
Keywords: BRAF; BRAF inhibitor; Disease progression; Immune checkpoint blockade; MEK inhibitor; Melanoma; NRAS; Nodal relapse; Overall survival; Survival analysis.
Conflict of interest statement
Ethics approval and consent to participate
This retrospective analysis was approved by the institutional review board of the medical faculty of the Munich University Hospital. The design of the study was exclusively retrospective and all data that were used in this report were extracted from pre-existing routine patient records. All treatment decisions were made by the treating oncologists and entirely independent of this analysis. No additional data were obtained at any time during the data collection. For this design, the ethics committee did not require informed consent obtained by each patient. As part of the routine treatment information and consent, all patients provided signed informed consent before they started systemic treatment or underwent any invasive procedure. The study followed the principles of the Declaration of Helsinki and of good clinical practice.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Bauer J, Buttner P, Murali R, Okamoto I, Kolaitis NA, Landi MT, et al. BRAF mutations in cutaneous melanoma are independently associated with age, anatomic site of the primary tumor, and the degree of solar elastosis at the primary tumor site. Pigment Cell Melanoma Res. 2011;24(2):345–351. doi: 10.1111/j.1755-148X.2011.00837.x. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
