

Measuring the impact of seasonal malaria chemoprevention as part of routine malaria control in Kita, Mali
- PMID: 28797263
- PMCID: PMC5553795
- DOI: 10.1186/s12936-017-1974-x
Measuring the impact of seasonal malaria chemoprevention as part of routine malaria control in Kita, Mali
Abstract
Background: Seasonal malaria chemoprevention (SMC) is a new strategy recommended by WHO in areas of highly seasonal transmission in March 2012. Although randomized controlled trials (RCTs) have shown SMC to be highly effective, evidence and experience from routine implementation of SMC are limited.
Methods: A non-randomized pragmatic trial with pre-post design was used, with one intervention district (Kita), where four rounds of SMC with sulfadoxine + amodiaquine (SP + AQ) took place in August-November 2014, and one comparison district (Bafoulabe). The primary aims were to evaluate SMC coverage and reductions in prevalence of malaria and anaemia when SMC is delivered through routine programmes using existing community health workers. Children aged 3-59 months from 15 selected localities per district, sampled with probability proportional to size, were surveyed and blood samples collected for malaria blood smears, haemoglobin (Hb) measurement, and molecular markers of drug resistance in two cross-sectional surveys, one before SMC (July 2014) and one after SMC (December 2014). Difference-in-differences regression models were used to assess and compare changes in malaria and anaemia in the intervention and comparison districts. Adherence and tolerability of SMC were assessed by cross-sectional surveys 4-7 days after each SMC round. Coverage of SMC was assessed in the post-SMC survey.
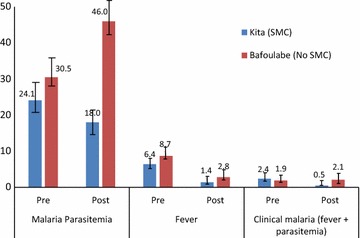
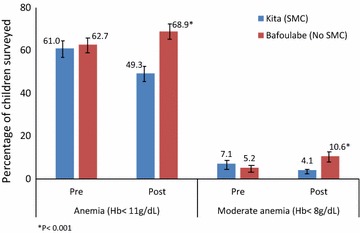
Results: During round 1, 84% of targeted children received at least the first SMC dose, but coverage declined to 67% by round 4. Across the four treatment rounds, 54% of children received four complete SMC courses. Prevalence of parasitaemia was similar in intervention and comparison districts prior to SMC (23.4 vs 29.5%, p = 0.34) as was the prevalence of malaria illness (2.4 vs 1.9%, p = 0.75). After SMC, parasitaemia prevalence fell to 18% in the intervention district and increased to 46% in the comparison district [difference-in-differences (DD) OR = 0.35; 95% CI 0.20-0.60]. Prevalence of malaria illness fell to a greater degree in the intervention district versus the comparison district (DD OR = 0.20; 95% CI 0.04-0.94) and the same for moderate anaemia (Hb < 8 g/dL) (DD OR = 0.26, 95% CI 0.11-0.65). The frequency of the quintuple mutation (dhfr N51I, C59R and S108N + dhps A437G and K540E) remained low (5%) before and after intervention in both districts.
Conclusions: Routine implementation of SMC in Mali substantially reduced malaria and anaemia, with reductions of similar magnitude to those seen in previous RCTs. Improving coverage could further strengthen SMC impact. Trial registration clinical trial registration number NCT02894294.
Figures
Similar articles
-
Effect of seasonal malaria chemoprevention in children between 5 and 9 years old in Kita and Bafoulabe districts, Mali.Parasite Epidemiol Control. 2022 Jun 22;18:e00258. doi: 10.1016/j.parepi.2022.e00258. eCollection 2022 Aug. Parasite Epidemiol Control. 2022. PMID: 35789762 Free PMC article. Review.
-
Cost-effectiveness of district-wide seasonal malaria chemoprevention when implemented through routine malaria control programme in Kita, Mali using fixed point distribution.Malar J. 2021 Mar 4;20(1):128. doi: 10.1186/s12936-021-03653-x. Malar J. 2021. PMID: 33663488 Free PMC article.
-
Effectiveness of Seasonal Malaria Chemoprevention in Children under Ten Years of Age in Senegal: A Stepped-Wedge Cluster-Randomised Trial.PLoS Med. 2016 Nov 22;13(11):e1002175. doi: 10.1371/journal.pmed.1002175. eCollection 2016 Nov. PLoS Med. 2016. PMID: 27875528 Free PMC article. Clinical Trial.
-
Evaluation of seasonal malaria chemoprevention in two areas of intense seasonal malaria transmission: Secondary analysis of a household-randomised, placebo-controlled trial in Houndé District, Burkina Faso and Bougouni District, Mali.PLoS Med. 2020 Aug 21;17(8):e1003214. doi: 10.1371/journal.pmed.1003214. eCollection 2020 Aug. PLoS Med. 2020. PMID: 32822362 Free PMC article. Clinical Trial.
-
Systematic Review and Meta-Analysis of Seasonal Malaria Chemoprevention.Am J Trop Med Hyg. 2023 Dec 11;110(1):20-31. doi: 10.4269/ajtmh.23-0481. Print 2024 Jan 3. Am J Trop Med Hyg. 2023. PMID: 38081050 Free PMC article.
Cited by
-
Prognostics of multiple malaria episodes and nutritional status in children aged 6 to 59 months from 2013 to 2017 in Dangassa, Mali.Res Sq [Preprint]. 2023 Nov 15:rs.3.rs-3604955. doi: 10.21203/rs.3.rs-3604955/v1. Res Sq. 2023. Update in: Malar J. 2024 Jun 13;23(1):186. doi: 10.1186/s12936-024-04999-8. PMID: 38014243 Free PMC article. Updated. Preprint.
-
Effect of a fifth round of seasonal malaria chemoprevention in children aged 5-14 years in Dangassa, an area of long transmission in Mali.Parasite Epidemiol Control. 2023 Jan 2;20:e00283. doi: 10.1016/j.parepi.2022.e00283. eCollection 2023 Feb. Parasite Epidemiol Control. 2023. PMID: 36704118 Free PMC article.
-
Barriers to the quality delivery of seasonal malaria chemoprevention in Chad and Burkina Faso: a qualitative exploration of caregivers and community distributors' perspectives.Malar J. 2024 Jul 19;23(1):216. doi: 10.1186/s12936-024-05034-6. Malar J. 2024. PMID: 39030554 Free PMC article.
-
Malaria chemoprevention and drug resistance: a review of the literature and policy implications.Malar J. 2022 Mar 24;21(1):104. doi: 10.1186/s12936-022-04115-8. Malar J. 2022. PMID: 35331231 Free PMC article. Review.
-
Effect of routine seasonal malaria chemoprevention on malaria trends in children under 5 years in Dangassa, Mali.Malar J. 2020 Apr 6;19(1):137. doi: 10.1186/s12936-020-03202-y. Malar J. 2020. PMID: 32252774 Free PMC article.
References
-
- WHO . World malaria report 2015. Geneva: World Health Organization; 2015.
-
- Repubique du Mali. Enquête sur les indicateurs du paludisme (EIP) 2015. http://dhsprogram.com/pubs/pdf/PR69/PR69.pdf. Accessed Jun 2016.
-
- WHO . Policy recommendation: seasonal malaria chemoprevention (SMC) for Plasmodium falciparum malaria control in highly seasonal transmission areas of the Sahel sub-region in Africa. Geneva: World Health Organization; 2012.
-
- WHO. Seasonal malaria chemoprevention with sulfadoxine-pyrimethamine plus amodiaquine in children: a field guide. Geneva: World Health Organization; 2013. http://www.who.int/malaria/publications/atoz/9789241504737/en/. Accessed Jun 2016.
-
- Dicko A, Diallo AI, Tembine I, Dicko Y, Dara N, Sidibe Y, et al. Intermittent preventive treatment of malaria provides substantial protection against malaria in children already protected by an insecticide-treated bednet in Mali: a randomised, double-blind, placebo-controlled trial. PLoS Med. 2011;8:e1000407. doi: 10.1371/journal.pmed.1000407. - DOI - PMC - PubMed
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
