

Practical approach to the patient with acute neuromuscular weakness
- PMID: 28798922
- PMCID: PMC5535318
- DOI: 10.12998/wjcc.v5.i7.270
Practical approach to the patient with acute neuromuscular weakness
Abstract
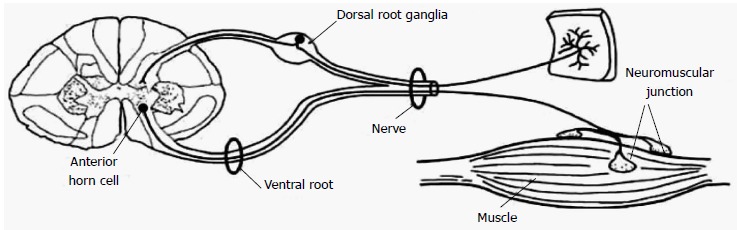
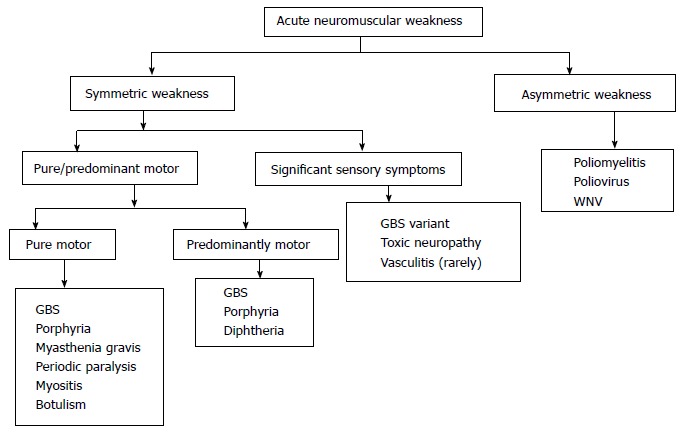
Acute neuromuscular paralysis (ANMP) is a clinical syndrome characterized by rapid onset muscle weakness progressing to maximum severity within several days to weeks (less than 4 wk). Bulbar and respiratory muscle weakness may or may not be present. It is a common neurological emergency which requires immediate and careful investigations to determine the etiology because accurate diagnosis has significant impact on therapy and prognosis. Respiratory failure caused by neuromuscular weakness is considered as more critical than lung disease because its development may be insidious or subtle until sudden decompensation leads to life threatening hypoxia. Also, the arterial blood gas finding of severe hypoxemia, hypercapnia, and acidosis may not be apparent until respiratory failure is profound. Hence, the requirement for respiratory assistance should also be intensively and promptly investigated in all patients with neuromuscular disease. The disorder is classified based on the site of defect in motor unit pathway, i.e., anterior horn cells, nerve root, peripheral nerve, neuromuscular junction or muscle. Identification of the cause is primarily based on a good medical history and detailed clinical examination supplemented with neurophysiologic investigations and sometimes few specific laboratory tests. Medical history and neurological examination should be focused on the onset, progression, pattern and severity of muscle weakness as well as cranial nerves testing and tests for autonomic dysfunction. Associated non neurological features like fever, rash or other skin lesions etc. should also be noted. Globally, Guillain-Barré syndrome is the most frequent cause of ANMP and accounts for the majority of cases of respiratory muscles weakness associated with neuromuscular disorders. Newly acquired neuromuscular weakness in intensive care unit patients consist of critical illness polyneuropathy, critical illness myopathy and drug induced neuromuscular weakness which may arise as a consequence of sepsis, multi-organ failure, and exposure to certain medications like intravenous corticosteroids and neuromuscular blocking agents.
Keywords: Approach; Muscle; Nerve; Neuromuscular weakness; Paralysis.
Conflict of interest statement
Conflict-of-interest statement: There is no conflict-of-interest.
Figures
References
-
- Maramattom BV, Wijdicks EF. Acute neuromuscular weakness in the intensive care unit. Crit Care Med. 2006;34:2835–2841. - PubMed
-
- Hutchinson D, Whyte K. Neuromuscular disease and respiratory failure. Pract Neurol. 2008;8:229–237. - PubMed
-
- Ropper AH. The Guillain-Barré syndrome. N Engl J Med. 1992;326:1130–1136. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
