

Developmental PBDE Exposure and IQ/ADHD in Childhood: A Systematic Review and Meta-analysis
- PMID: 28799918
- PMCID: PMC5783655
- DOI: 10.1289/EHP1632
Developmental PBDE Exposure and IQ/ADHD in Childhood: A Systematic Review and Meta-analysis
Abstract
Background: In the United States, one in six children are affected by neurodevelopmental disorders, and polybrominated diphenyl ethers (PBDEs) in flame-retardant chemicals are measured ubiquitously in children.
Objective: We conducted a systematic a systematic review regarding developmental exposure to PBDEs and intelligence or Attention Deficit/Hyperactivity Disorder (ADHD) and attention-related behavioral conditions in humans.
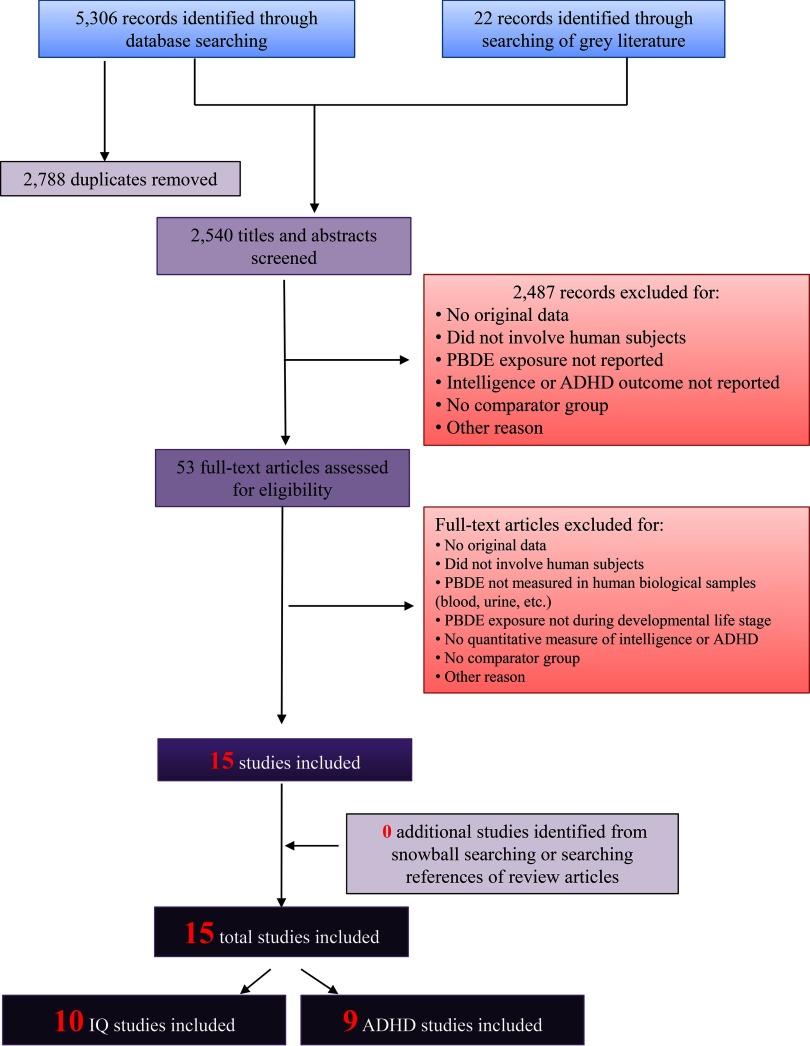
Methods: We searched articles published up to 26 September 2016, and included original studies that quantified exposures to PBDEs incurred any time in proximity to conception or during in utero, perinatal, or childhood time periods. We evaluated the risk of bias of individual studies and the overall quality and strength of the evidence according to the Navigation Guide systematic review methodology. We established criteria in advance to identify studies that could be combined using random effects meta-analyses (DerSimonian-Laird method).
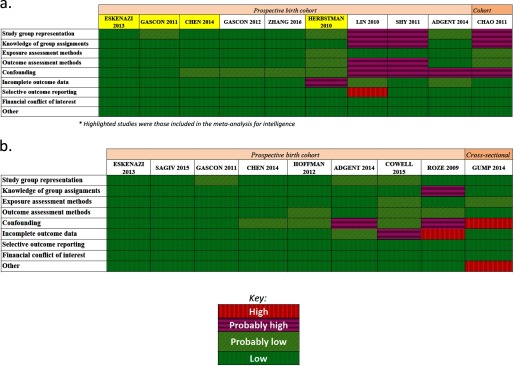
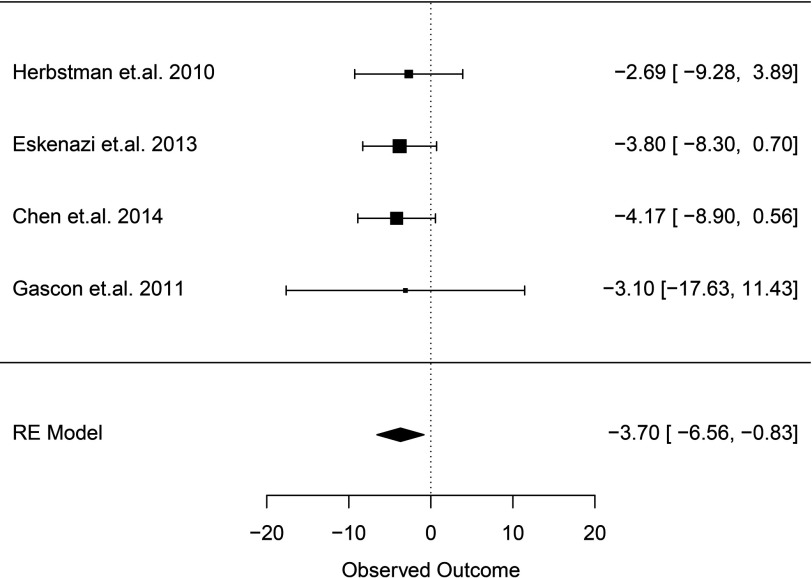
Results: Fifteen studies met the inclusion criteria; 10 studies met the criteria for intelligence and nine for attention-related problems. We rated studies generally with "low" to "probably low" risk of bias and rated the overall body of evidence as "moderate" quality with "sufficient" evidence for an association between Intelligence Quotient (IQ) and PBDEs. Our meta-analysis of four studies estimated a 10-fold increase (in other words, times 10) in PBDE exposure associated with a decrement of 3.70 IQ points (95% confidence interval: 0.83, 6.56). We concluded the body of evidence was of "moderate" quality for ADHD with "limited" evidence for an association with PBDEs, based on the heterogeneity of association estimates reported by a small number of studies and the fact that chance, bias, and confounding could not be ruled out with reasonable confidence.
Conclusion: We concluded there was sufficient evidence supporting an association between developmental PBDE exposure and reduced IQ. Preventing developmental exposure to PBDEs could help prevent loss of human intelligence. https://doi.org/10.1289/EHP1632.
Figures
References
-
- Ades AE, Caldwell DM, Reken S, Welton NJ, Sutton AJ, Dias S. 2012. NICE DSU technical support document 7: Evidence synthesis of treatment efficacy in decision making: a reviewer's checklist. The Decision Support Unit. London UK:National Institute for Health and Care Excellence, PMID: 27905719 - PubMed
-
- ATSDR (Agency for Toxic Substances and Disease Registry). 2004. Toxicological profile for polybrominated biphenyls and polybrominated diphenyl ethers. https://www.atsdr.cdc.gov/toxprofiles/tp68.pdf [accessed 20 March 2017].
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
