

Vertical Macular Asymmetry Measures Derived From SD-OCT for Detection of Early Glaucoma
- PMID: 28800651
- PMCID: PMC5555252
- DOI: 10.1167/iovs.17-21961
Vertical Macular Asymmetry Measures Derived From SD-OCT for Detection of Early Glaucoma
Erratum in
-
Erratum.Invest Ophthalmol Vis Sci. 2017 Sep 1;58(11):4799. doi: 10.1167/iovs.17-22948a. Invest Ophthalmol Vis Sci. 2017. PMID: 28973336 Free PMC article. No abstract available.
Abstract
Purpose: To test the hypothesis that vertical asymmetry in macular ganglion cell/inner plexiform layer (GCIPL) thickness can improve detection of early glaucoma.
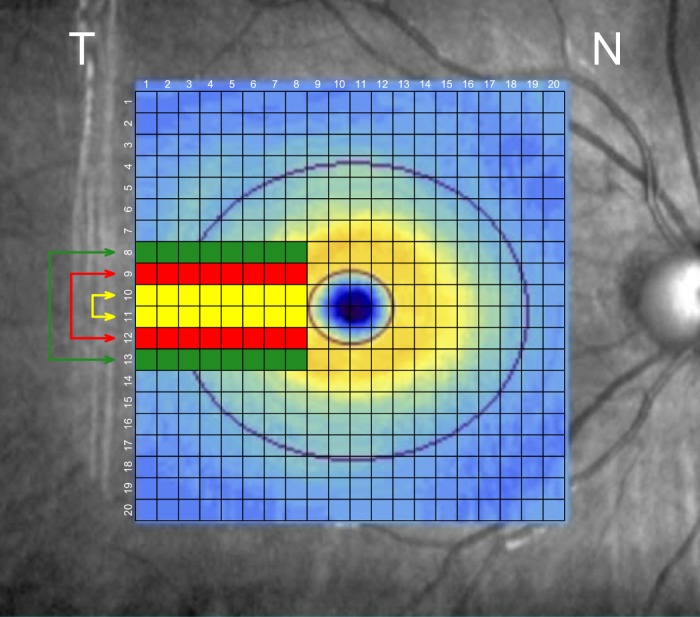
Methods: Sixty-nine normal eyes and 101 glaucoma eyes had macular imaging with spectral-domain optical coherence tomography (OCT; 200 × 200 cube). The resulting GCIPL thickness matrix was grouped into a 20 × 20 superpixel array and superior superpixels were compared to their inferior counterparts. A global asymmetry index (AI) was defined as the grand mean of the asymmetry ratios. To measure local asymmetry, the corresponding thickness measurements of three rows above and below the horizontal raphe were compared individually and in combinations. Global and local AIs were compared to the best-performing GCIPL thickness parameters with area under the receiver operating curves (AUC) and sensitivity/specificities.
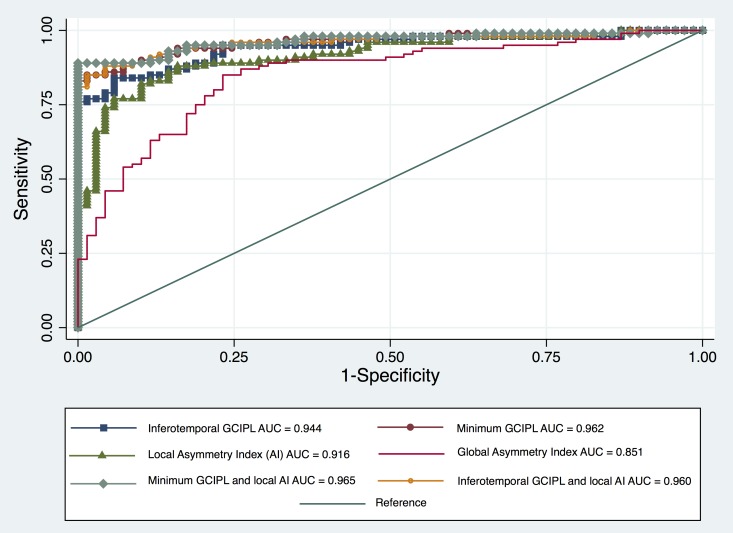
Results: Age or axial length did not influence AIs in normal subjects (P ≥ 0.08). Global and local AIs were significantly higher in the glaucoma group compared to normal eyes. Minimum (AUC = 0.962, 95% confidence interval [CI]: 0.936-0.989) and inferotemporal thickness (AUC = 0.944, 95% CI: 0.910-0.977; P = 0.122) performed best for detection of early glaucoma. The AUC for global AI was 0.851 (95% CI: 0.792-0.909) compared to 0.916 (95% CI: 0.874-0.958) for the best local AI. Combining minimum or inferotemporal GCIPL thickness and the best local AI led to higher partial AUCs (0.088 and 0.085, 90% specificity, P = 0.120 and 0.130, respectively) than GCIPL thickness measures.
Conclusions: Macular vertical thickness asymmetry measures did not perform better than sectoral or minimum GCIPL thickness for detection of early glaucoma. Combining local asymmetry parameters with the best sectoral GCIPL thickness measures enhanced this task.
Figures
References
-
- Sommer A,, Miller NR,, Pollack I,, Maumenee AE,, George T. The nerve fiber layer in the diagnosis of glaucoma. Arch Ophthalmol. 1977; 95: 2149–2156. - PubMed
-
- Sommer A,, Katz J,, Quigley HA,, et al. Clinically detectable nerve fiber atrophy precedes the onset of glaucomatous field loss. Arch Ophthalmol. 1991; 109: 77–83. - PubMed
-
- Motolko M,, Drance SM. Features of the optic disc in preglaucomatous eyes. Arch Ophthalmol. 1981; 99: 1992–1994. - PubMed
-
- Tuulonen A,, Lehtola J,, Airaksinen PJ. Nerve fiber layer defects with normal visual fields. Do normal optic disc and normal visual field indicate absence of glaucomatous abnormality? Ophthalmology. 1993; 100: 587–597; discussion 597–598. - PubMed
-
- Kass MA,, Heuer DK,, Higginbotham EJ,, et al. The Ocular Hypertension Treatment study: a randomized trial determines that topical ocular hypotensive medication delays or prevents the onset of primary open-angle glaucoma. Arch Ophthalmol 2002; 120: 701–713; discussion 829–830. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
