

Levothyroxine enhances glucose clearance and blunts the onset of experimental type 1 diabetes mellitus in mice
- PMID: 28800677
- PMCID: PMC5647183
- DOI: 10.1111/bph.13975
Levothyroxine enhances glucose clearance and blunts the onset of experimental type 1 diabetes mellitus in mice
Abstract
Background and purpose: Thyroid hormones induce several changes in whole body metabolism that are known to improve metabolic homeostasis. However, adverse side effects have prevented its use in the clinic. In view of the promising effects of thyroid hormones, we investigated the effects of levothyroxine supplementation on glucose homeostasis.
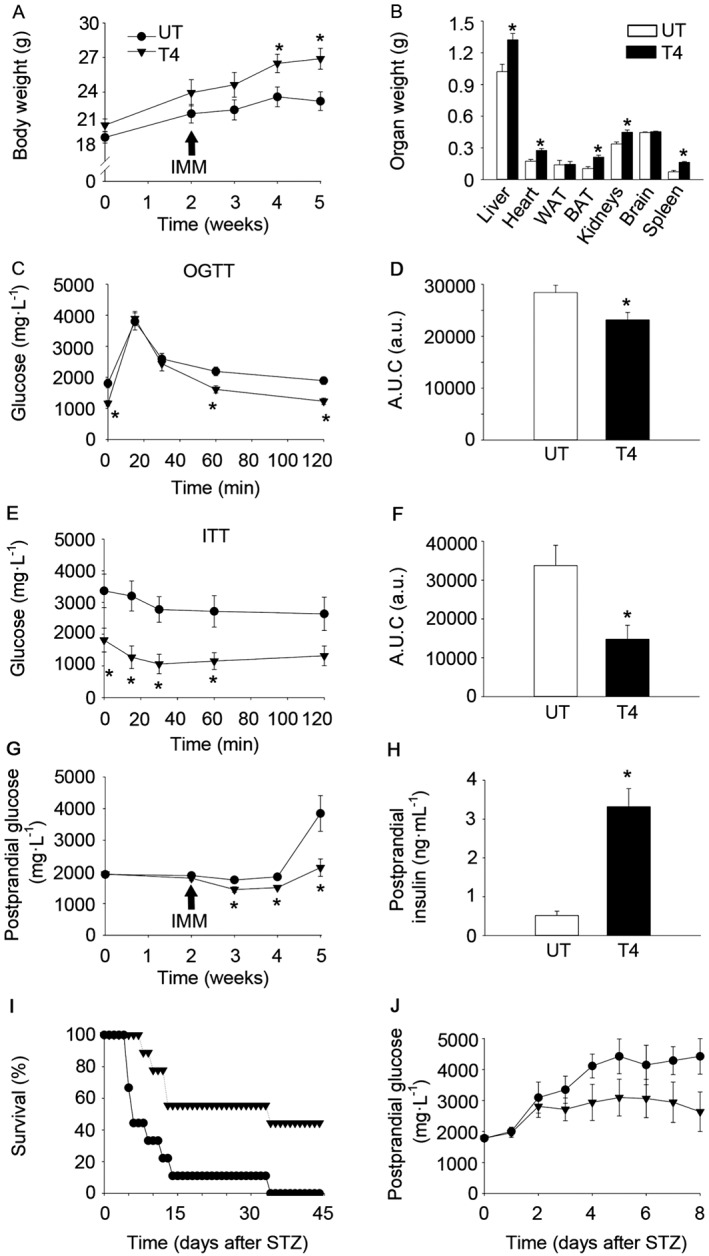
Experimental approach: C57BL/6 mice were treated with levothyroxine from birth to 24 weeks of age, when mice were killed. The effects of levothyroxine supplementation on metabolic health were determined. C57BL/6 mice treated with levothyroxine for 2 weeks and then challenged with streptozotocin to monitor survival. Mechanistic experiments were conducted in the pancreas, liver and skeletal muscle. RIP-B7.1 mice were treated with levothyroxine for 2 weeks and were subsequently immunized to trigger experimental autoimmune diabetes (EAD). Metabolic tests were performed. Mice were killed and metabolic tissues were extracted for immunohistological analyses.
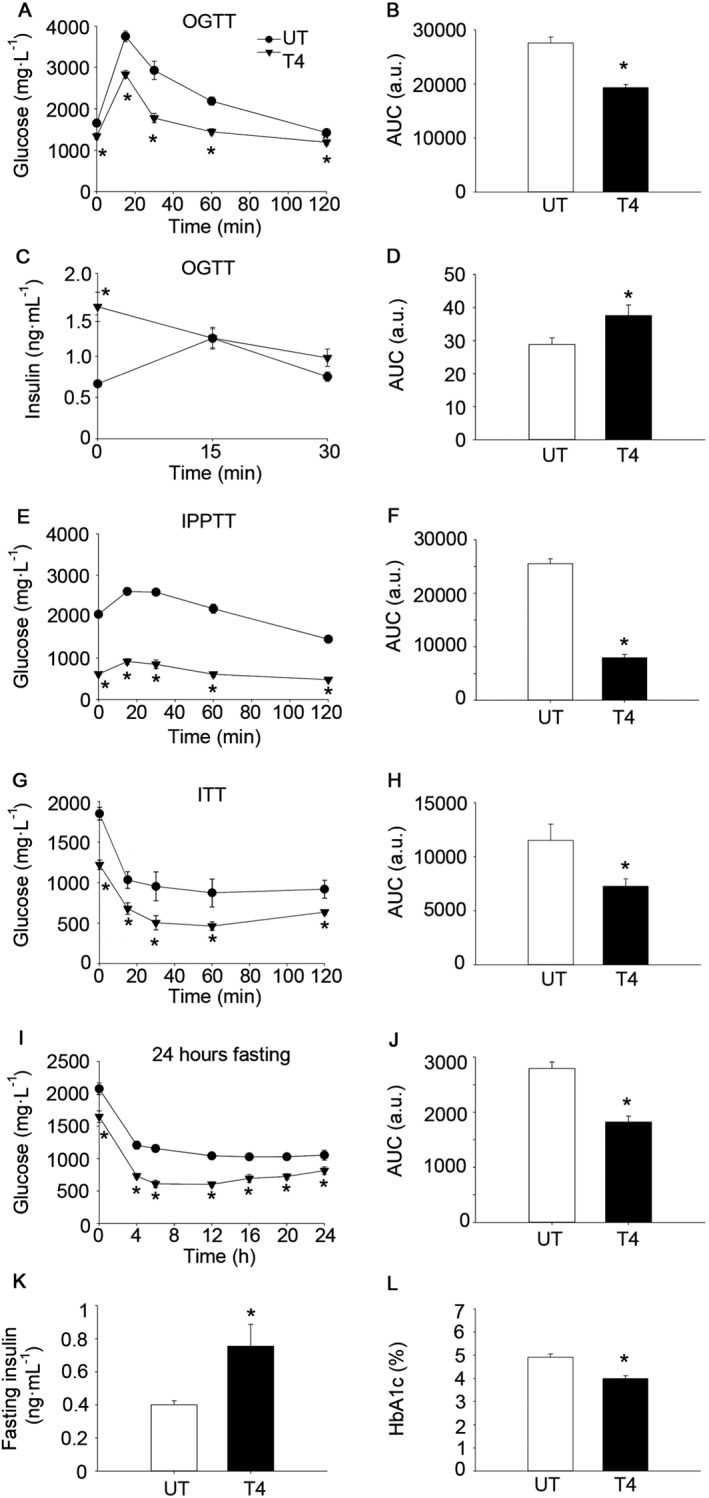
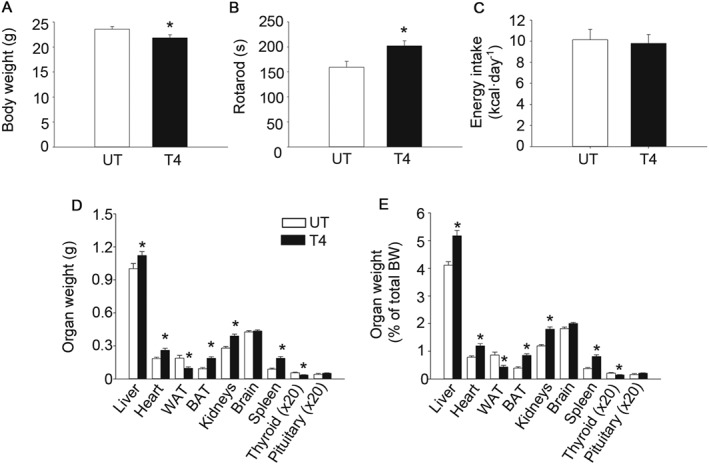
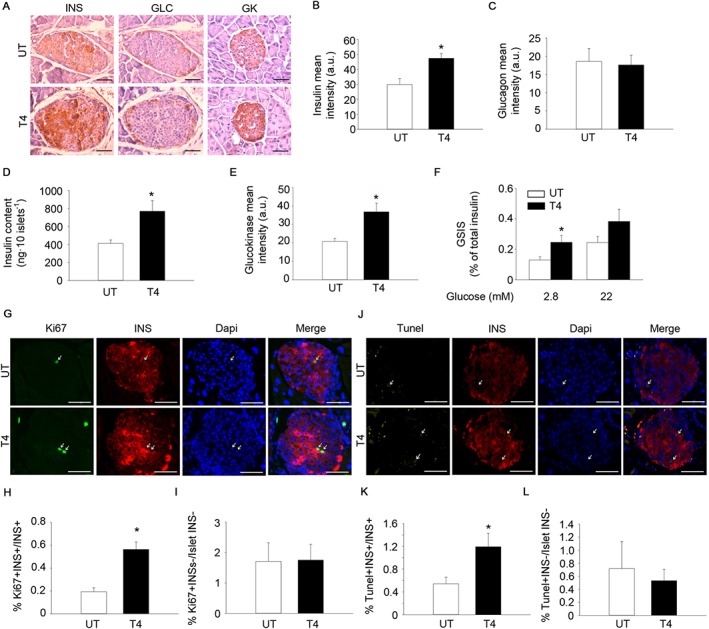
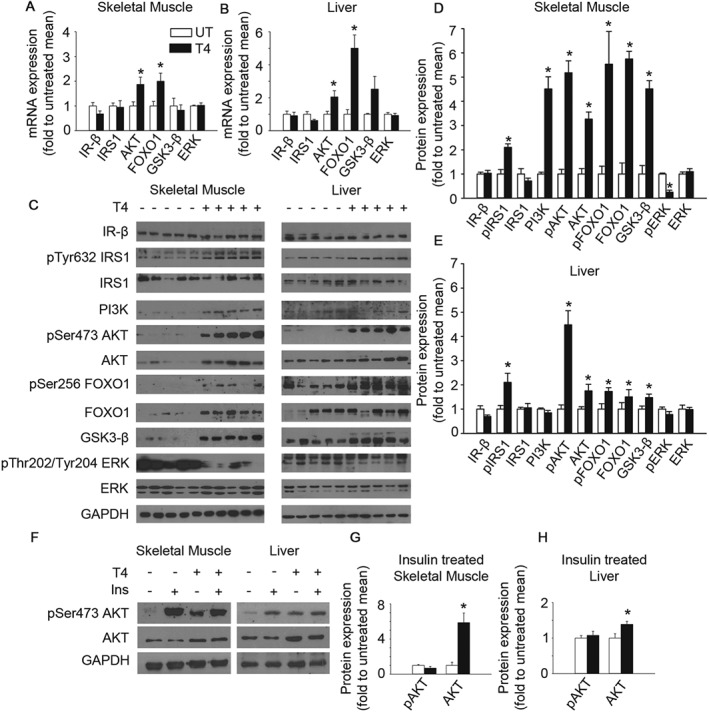
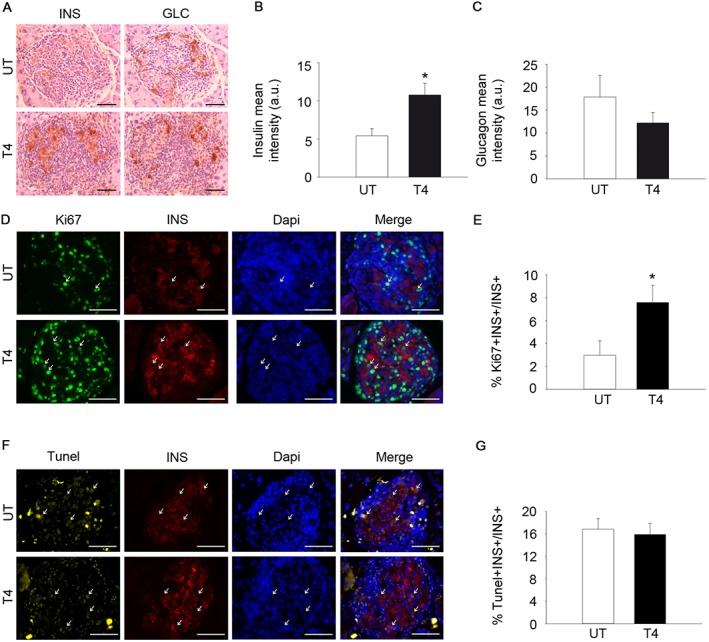
Key results: Long-term levothyroxine supplementation enhanced glucose clearance and reduced circulating glucose in C57BL/6 mice. Levothyroxine increased simultaneously the proliferation and apoptosis of pancreatic beta cells, promoting the maintenance of a highly insulin-expressing beta cell population. Levothyroxine increased circulating insulin levels, inducing sustained activation of IRS1-AKT signalling in insulin-target tissues. Levothyroxine-treated C57BL/6 mice challenged with streptozotocin exhibited extended survival. Levothyroxine blunted the onset of EAD in RIP-B7.1 mice by inducing beta cell proliferation and preservation of insulin-expressing cells.
Conclusions and implications: Interventions based on the use of thyroid hormones or thyromimetics could be explored to provide therapeutic benefit in patients with type 1 diabetes mellitus.
© 2017 The British Pharmacological Society.
Figures
References
-
- Aguayo‐Mazzucato C, Zavacki AM, Marinelarena A, Hollister‐Lock J, El Khattabi I, Marsili A et al (2013). Thyroid hormone promotes postnatal rat pancreatic beta‐cell development and glucose‐responsive insulin secretion through MAFA. Diabetes 62: 1569–1580. https://doi.org/10.2337/db12‐0849. - DOI - PMC - PubMed
-
- Aiello V, Moreno‐Asso A, Servitja JM, Martin M (2014). Thyroid hormones promote endocrine differentiation at expenses of exocrine tissue. Exp Cell Res 322: 236–248. https://doi.org/10.1016/j.yexcr.2014.01.030. - DOI - PubMed
-
- Bahn RS, Burch HB, Cooper DS, Garber JR, Greenlee MC, Klein I et al (2011). Hyperthyroidism and other causes of thyrotoxicosis: management guidelines of the American Thyroid Association and American Association of Clinical Endocrinologists. Endocr Pract 17: 456–520. https://doi.org/10.4158/EP.17.3.456. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
