

Cutaneous T-cell Lymphoma
- PMID: 28802499
- PMCID: PMC5710803
- DOI: 10.1016/j.cll.2017.06.006
Cutaneous T-cell Lymphoma
Abstract
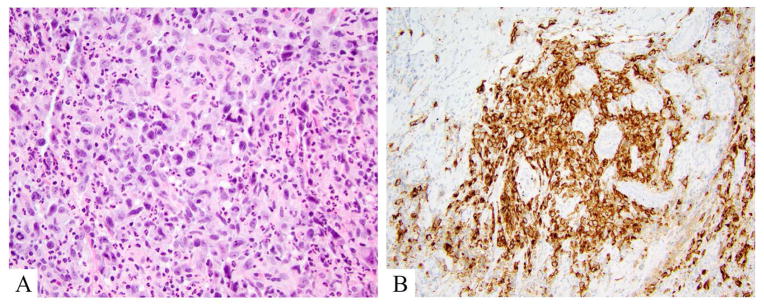
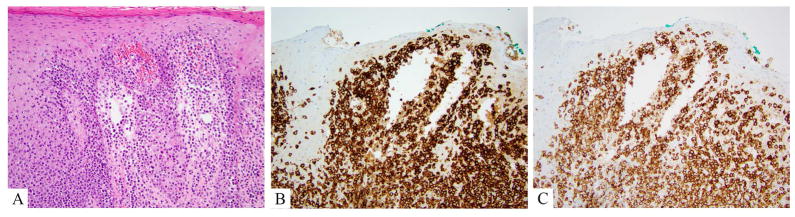
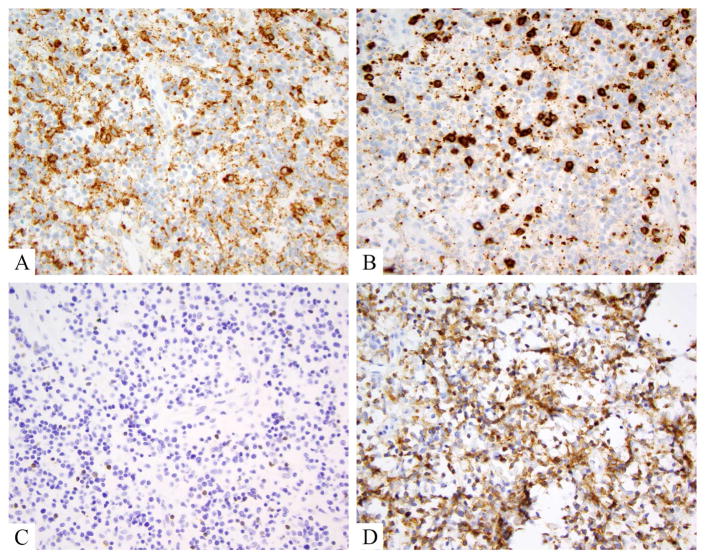
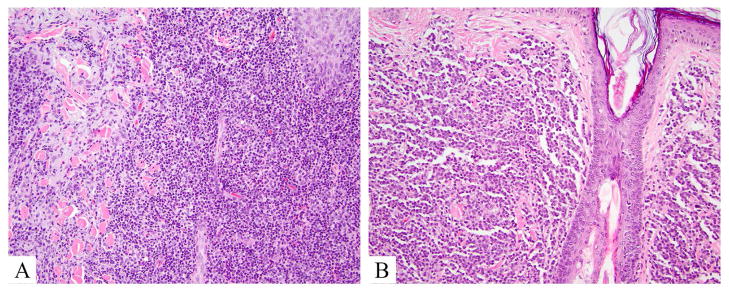
Cutaneous T-cell lymphomas comprise a heterogeneous group of diseases characterized by monoclonal proliferations of T lymphocytes primarily involving skin, modified skin appendages, and some mucosal sites. This article addresses the basic clinical, histologic, and immunohistochemical characteristics of this group of diseases, with additional attention to evolving literature on dermoscopy, reflectance confocal microscopy, flow cytometry, and molecular data that may increasingly be applied to diagnostic and therapeutic algorithms in these diseases. Select unusual phenotypes or diagnostic examples of classic phenotypes are demonstrated, and flags for consideration while making a pathologic diagnosis of cutaneous T-cell lymphoma are suggested.
Keywords: Anaplastic large cell lymphoma; Cutaneous lymphoma; Flow cytometry; Lymphomatoid papulosis; Mycosis fungoides; Reflective confocal microscopy; Sézary syndrome.
Copyright © 2017 Elsevier Inc. All rights reserved.
Figures
References
-
- Willemze R, et al. WHO-EORTC classification for cutaneous lymphomas. Blood. 2005;105(10):3768–85. - PubMed
-
- Swerdlow SH, EC, Harris NL, Jaffe ES. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. 4. Lyon, France: IARC Press; 2008.
-
- Beltraminelli H, et al. Primary cutaneous CD4+ small-/medium-sized pleomorphic T-cell lymphoma: a cutaneous nodular proliferation of pleomorphic T lymphocytes of undetermined significance? A study of 136 cases. Am J Dermatopathol. 2009;31(4):317–22. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
