

The Impact of Western Diet and Nutrients on the Microbiota and Immune Response at Mucosal Interfaces
- PMID: 28804483
- PMCID: PMC5532387
- DOI: 10.3389/fimmu.2017.00838
The Impact of Western Diet and Nutrients on the Microbiota and Immune Response at Mucosal Interfaces
Abstract
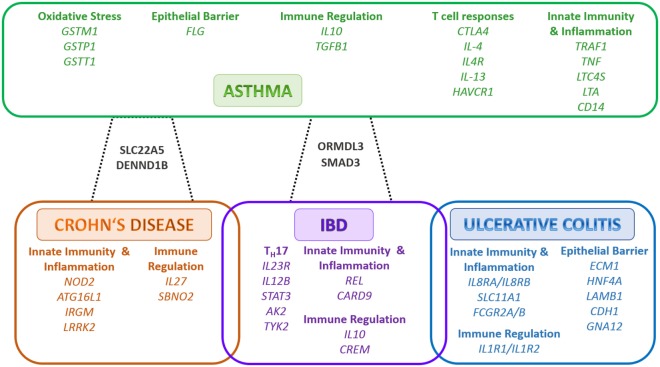
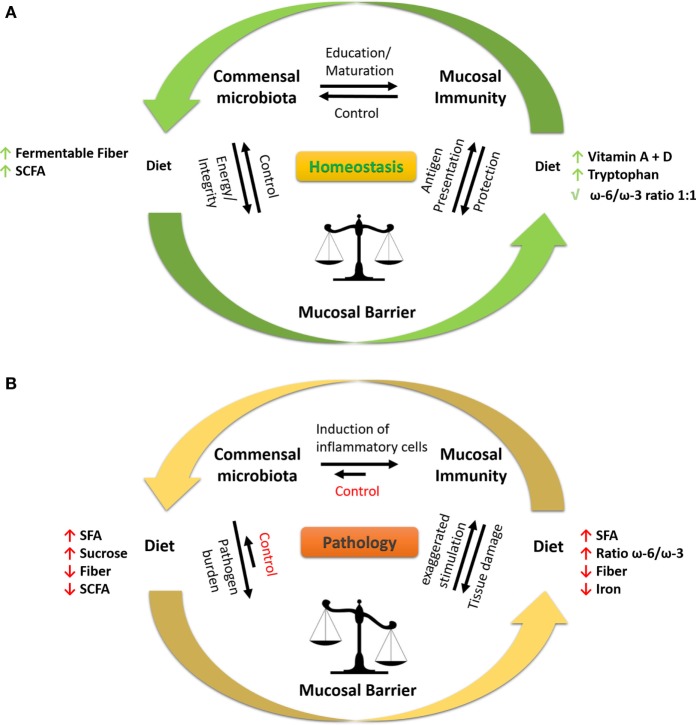
Recent findings point toward diet having a major impact on human health. Diets can either affect the gut microbiota resulting in alterations in the host's physiological responses or by directly targeting the host response. The microbial community in the mammalian gut is a complex and dynamic system crucial for the development and maturation of both systemic and mucosal immune responses. Therefore, the complex interaction between available nutrients, the microbiota, and the immune system are central regulators in maintaining homeostasis and fighting against invading pathogens at mucosal sites. Westernized diet, defined as high dietary intake of saturated fats and sucrose and low intake of fiber, represent a growing health risk contributing to the increased occurrence of metabolic diseases, e.g., diabetes and obesity in countries adapting a westernized lifestyle. Inflammatory bowel diseases (IBD) and asthma are chronic mucosal inflammatory conditions of unknown etiology with increasing prevalence worldwide. These conditions have a multifactorial etiology including genetic factors, environmental factors, and dysregulated immune responses. Their increased prevalence cannot solely be attributed to genetic considerations implying that other factors such as diet can be a major contributor. Recent reports indicate that the gut microbiota and modifications thereof, due to a consumption of a diet high in saturated fats and low in fibers, can trigger factors regulating the development and/or progression of both conditions. While asthma is a disease of the airways, increasing evidence indicates a link between the gut and airways in disease development. Herein, we provide a comprehensive review on the impact of westernized diet and associated nutrients on immune cell responses and the microbiota and how these can influence the pathology of IBD and asthma.
Keywords: asthma; inflammatory bowel disease; microbiota; micronutrients; saturated fat; westernized diet.
Figures
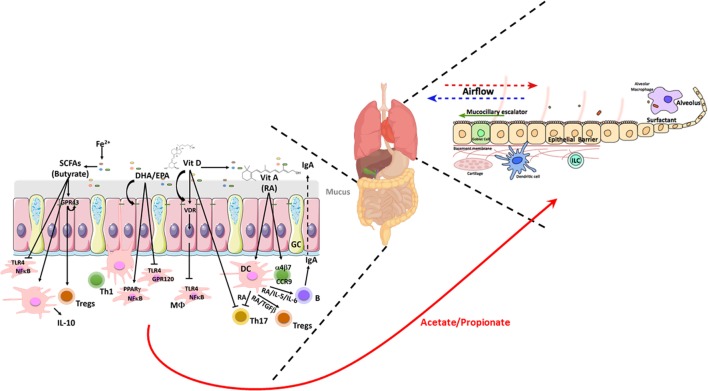
 , bacteroides;
, bacteroides;  , firmicutes;
, firmicutes;  , barrier integrity.
, barrier integrity.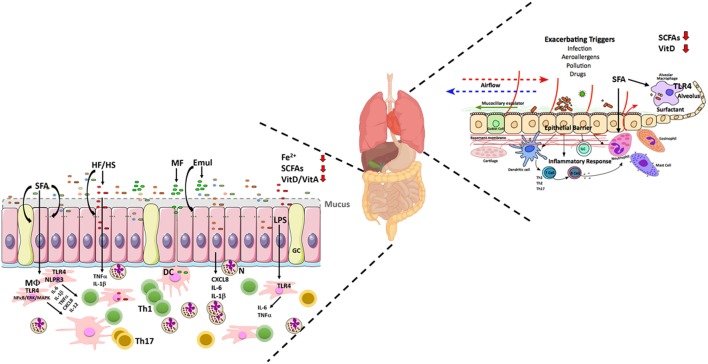
 , bacteroides;
, bacteroides;  , firmicutes;
, firmicutes;  , adherent and invasive Escherichia coli (AIEC);
, adherent and invasive Escherichia coli (AIEC);  , Bilophila wadsworthia;
, Bilophila wadsworthia;  , other altered bacterial spp;
, other altered bacterial spp;  , compromised barrier integrity.
, compromised barrier integrity.References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical